Figures
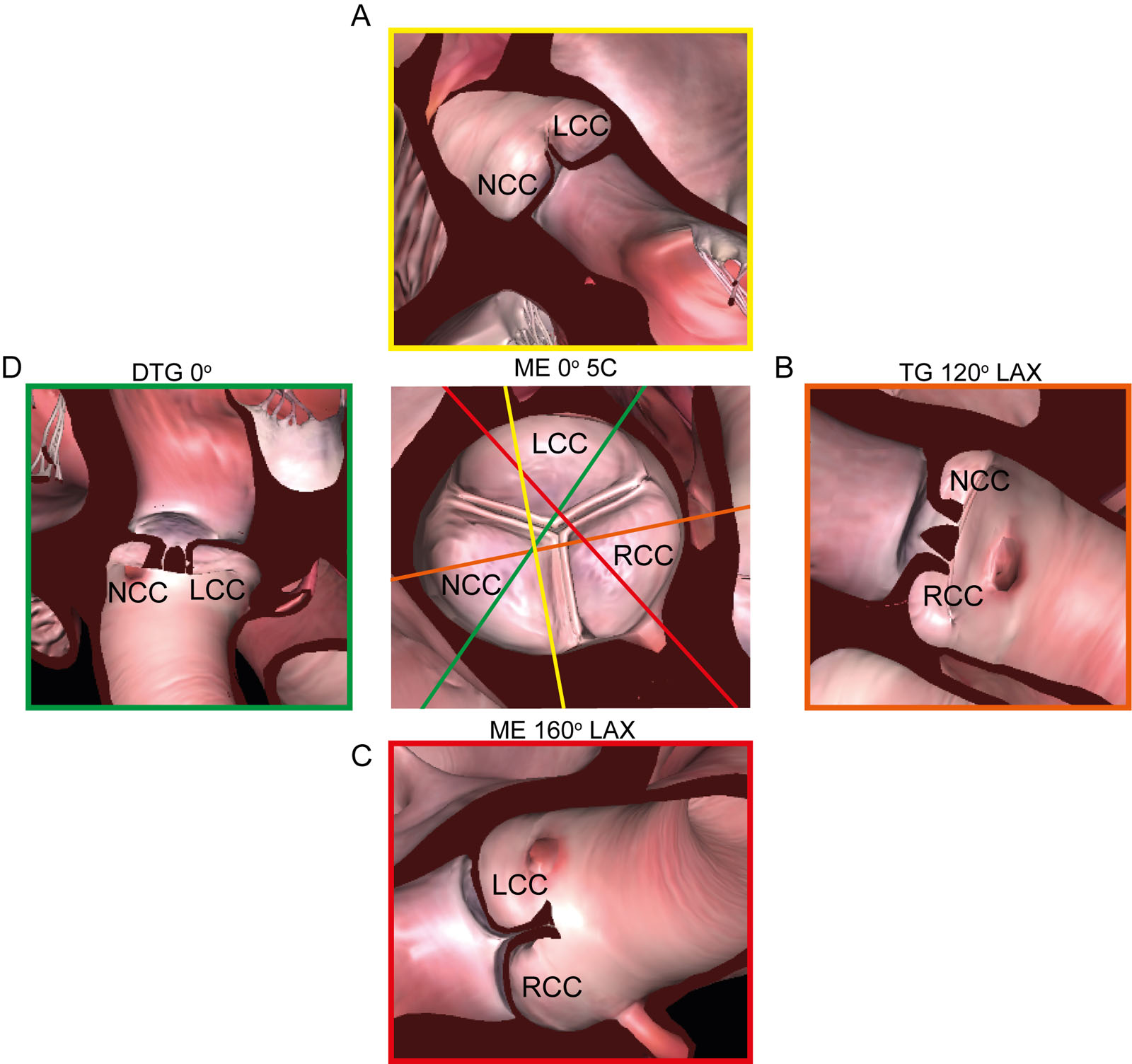
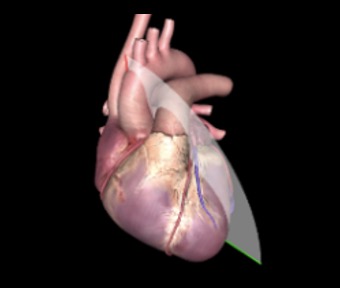
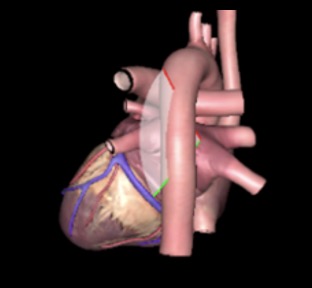
eFigure 14.7
AoV and 2D TEE views. This diagram shows the relationship of ME, TG and DTG TEE views to the AoV cusps. Abbreviations: 2D, two-dimensional; 5C, five-chamber; AoV, aortic valve; DTG, deep transgastric; LAX, long-axis; LCC left coronary cusp; ME, mid-esophageal; NCC, non-coronary cusp; RCC, right coronary cusp; TEE, transesophageal echocardiography; TG, transgastric.
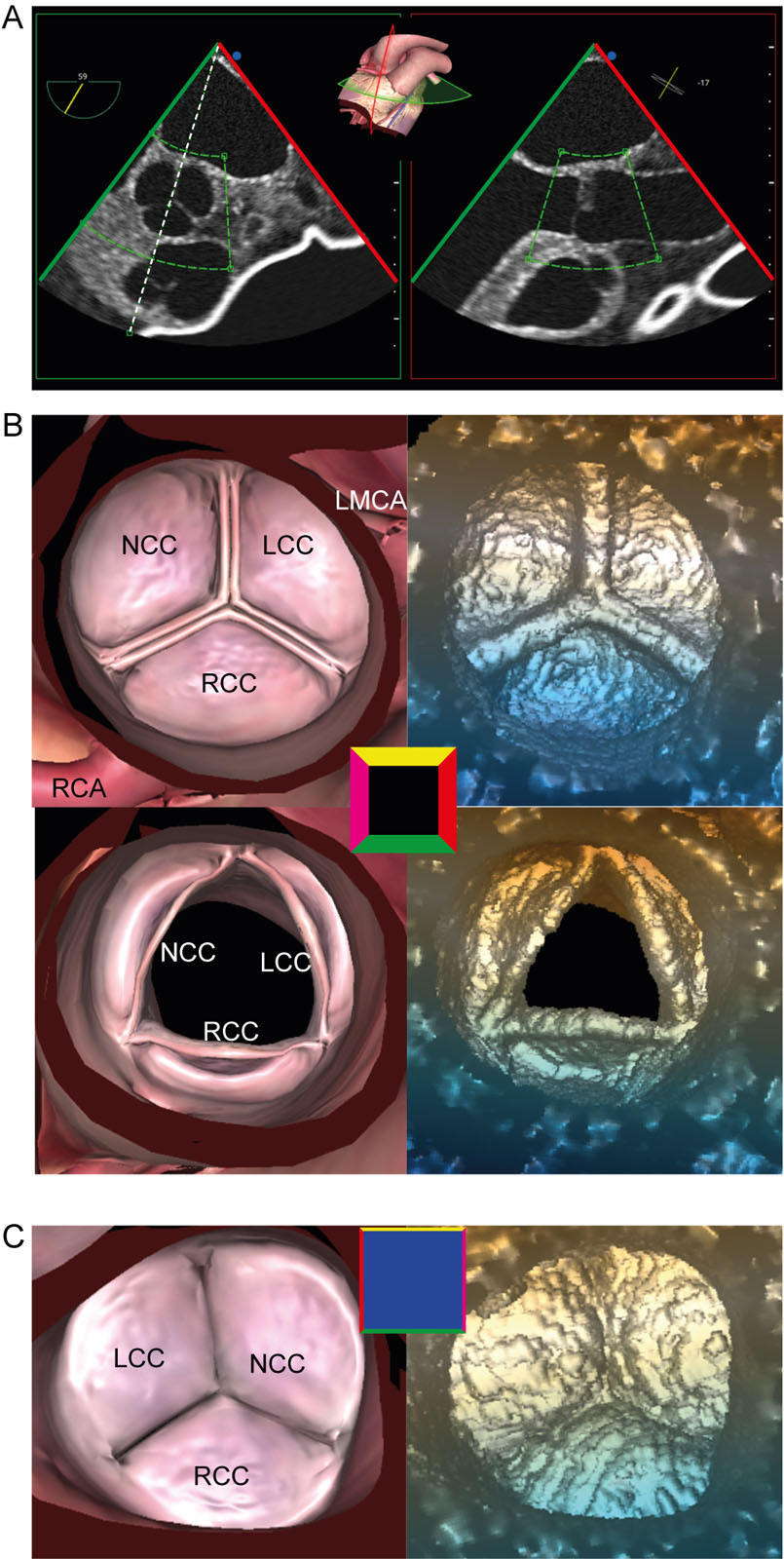
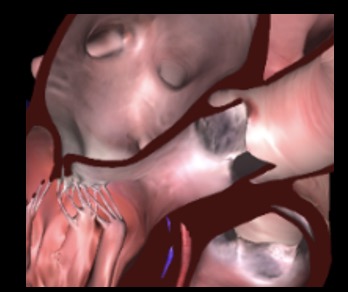
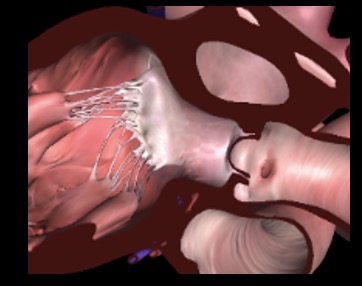
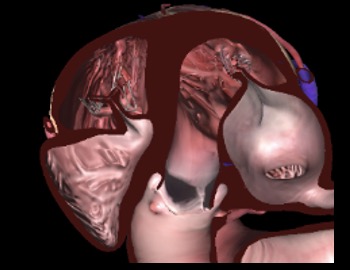
eFigure 14.10
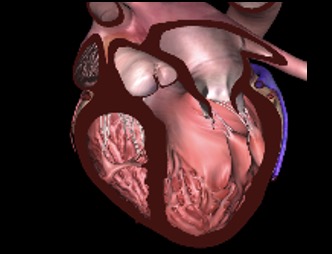
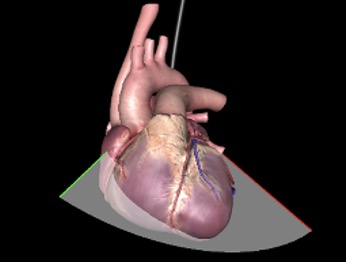
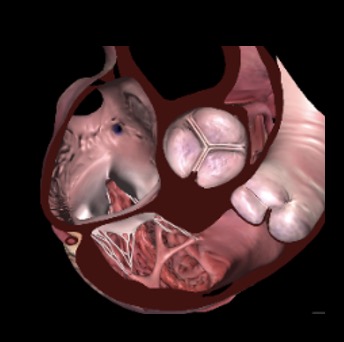
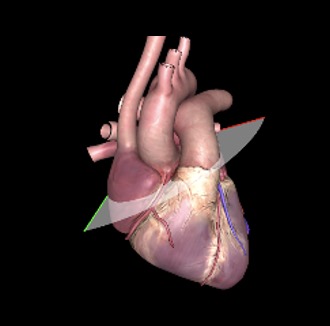
AoV 3D zoom acquisition. (A) 3D zoom acquisition beginning in the ME AoV SAX view should include all three AoV cusps and part of the LVOT and Asc Ao. (B) The 3D AoV dataset appears from the aortic perspective in diastole and systole. (C) A 180° rotation allows visualisation of the AoV from the LV perspective. Abbreviations: 3D, three-dimensional, AoV, aortic valve; Asc Ao, ascending aorta; LCC, left coronary cusp; LMCA, left main coronary artery; LV, left ventricular outflow tract; ME, mid-esophageal; NCC, non-coronary cusp; RCA, right coronary artery; RCC, right coronary cusp; SAX, short-axis.
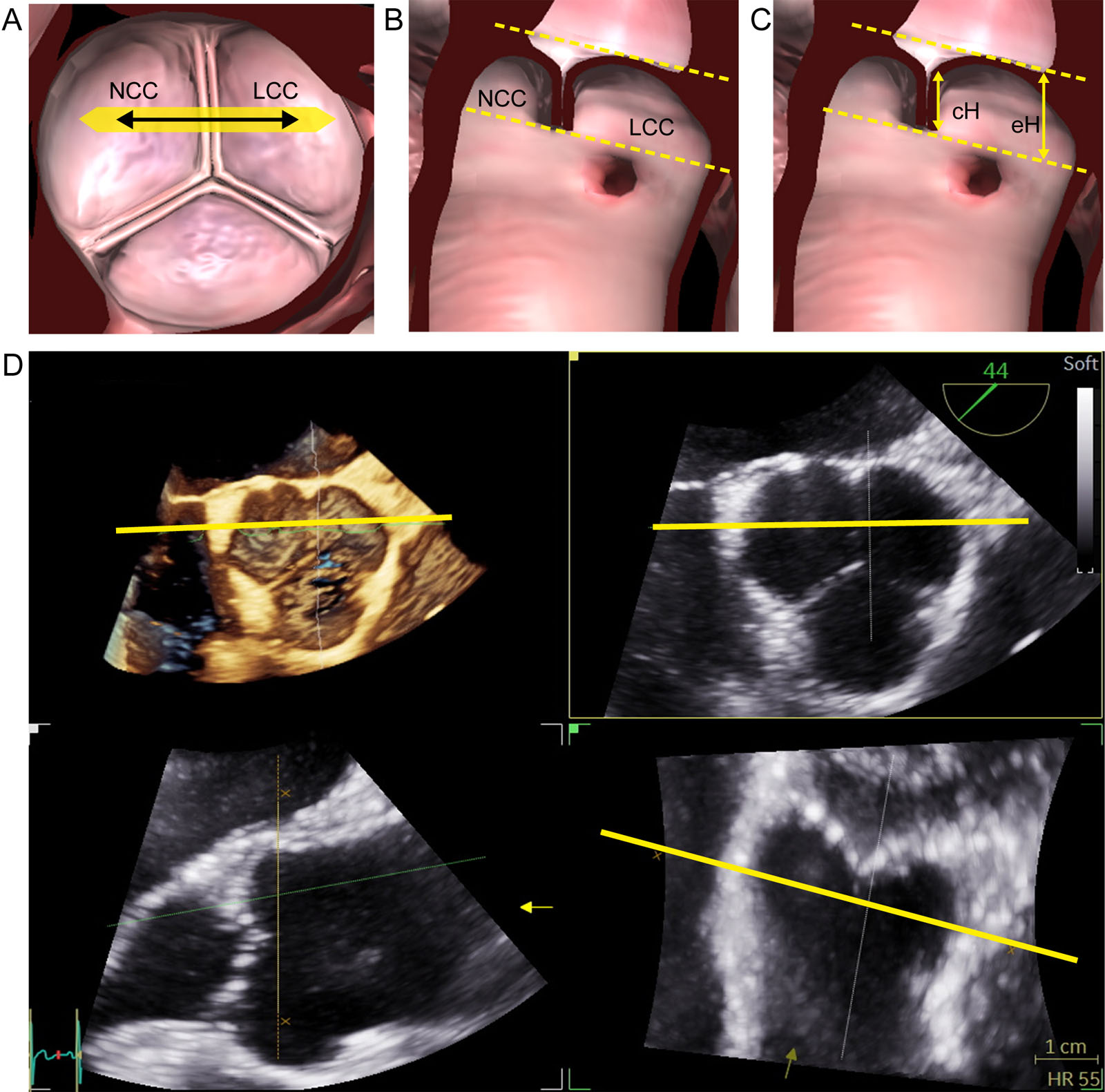
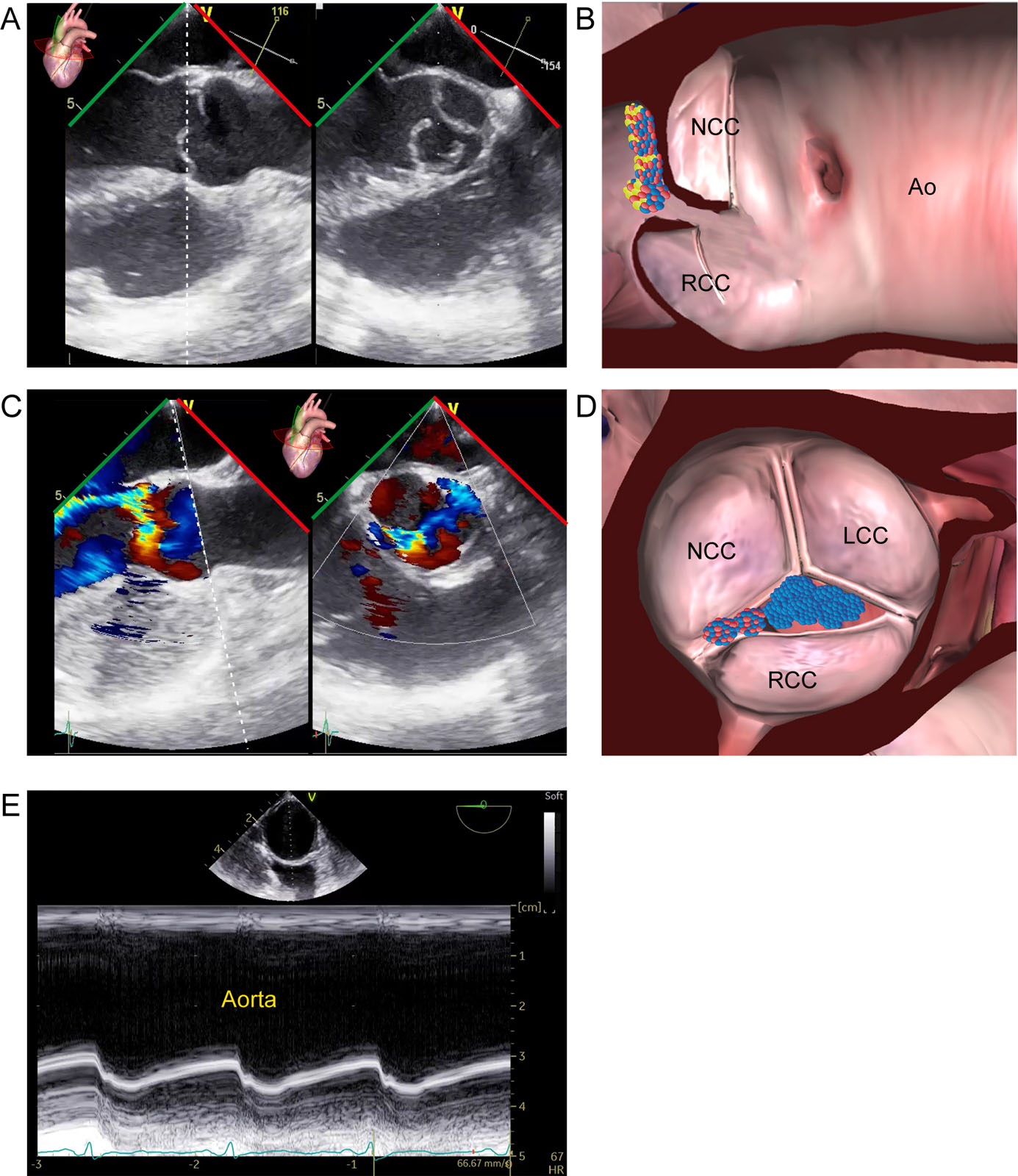
eFigure 14.14
AoV eH and cH measurements of NCC and LCC. (A-C) Measurements are taken between the respective cusps of a normal tricuspid AoV at the inner third of each commissure in the correct adjusted sectional plane. The orthogonal sectional planes through the center of the AoV must be adjusted perpendicular to the commissures between 2 respective cusps. The cH and eH positions between the NCC and the LCC are shown. (D) Corresponding 3D ME SAX view of the AoV with MPR. Abbreviations: 3D, three-dimensional; AoV, aortic valve; cH, coaptation height; eH, effective height; LCC, left coronary cusp; ME, mid-esophageal; MPR, multiplane reconstruction; NCC, non-coronary cusp; SAX, short-axis. Adapted from Hagendorff et al. 2
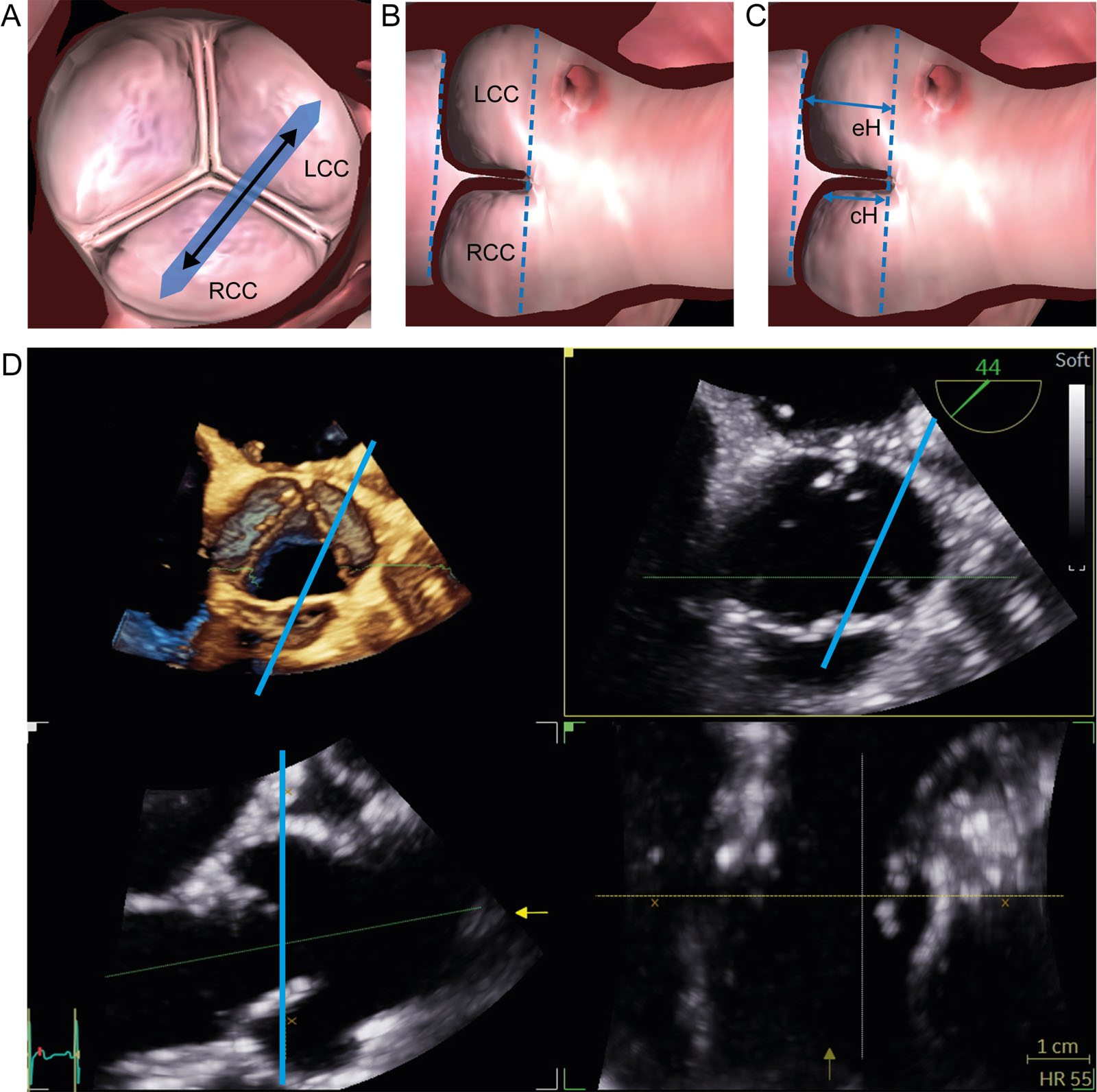
eFigure 14.15
Aortic valve eH and cH measurements of NCC and RCC. (A-C) Measurements should be taken between the respective cusps of a normal tricuspid AoV at the inner third of each commissure in the correct adjusted sectional plane. The orthogonal sectional planes through the AoV center must be adjusted perpendicular to the commissures between 2 respective cusps. The cH and eH positions between the RCC and the LCC appear. (D) Corresponding 3D ME SAX view of the AoV with MPR. Abbreviations: 3D, three-dimensional; AoV, aortic valve; cH, coaptation height; eH, effective height; LCC, left coronary cusp; ME, mid-esophageal; MPR, multiplane reconstruction; RCC, right coronary cusp; SAX, short-axis. Adapted from Hagendorf et al. 2
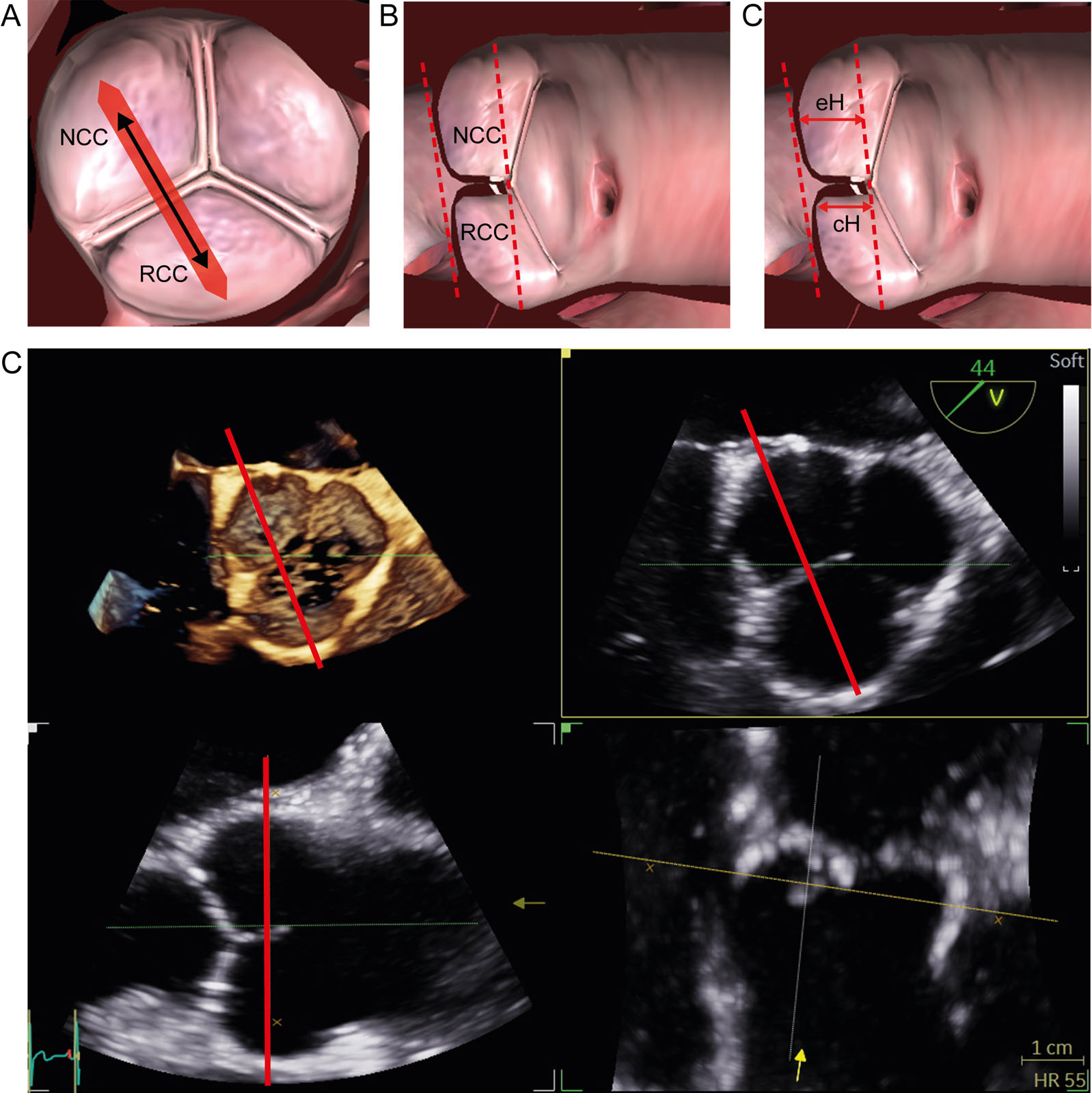
eFigure 14.16
Figure 14.17 AoV eH and cH measurements of RCCand NCC. (A-C) Measurements should be taken between the respective cusps of a normal tricuspid AoV at the inner third of each commissure in the correct adjusted sectional plane. The orthogonal sectional planes through the AoV center must be adjusted perpendicular to the commissures between 2 respective cusps. The cH and eH positions between the NCC and the RCC appear. (D) Corresponding 3D ME SAX view of the AoV with MPR. Abbreviations: 3D, three-dimensional; AoV, aortic valve; cH, coaptation height; eH, effective height; ME, mid-esophageal; MPR, multiplane reconstruction; NCC, non-coronary cusp; RCC where, right coronary cusp; SAX, short-axis. Adapted from Hagendorff et al.2
eFigure 14.25
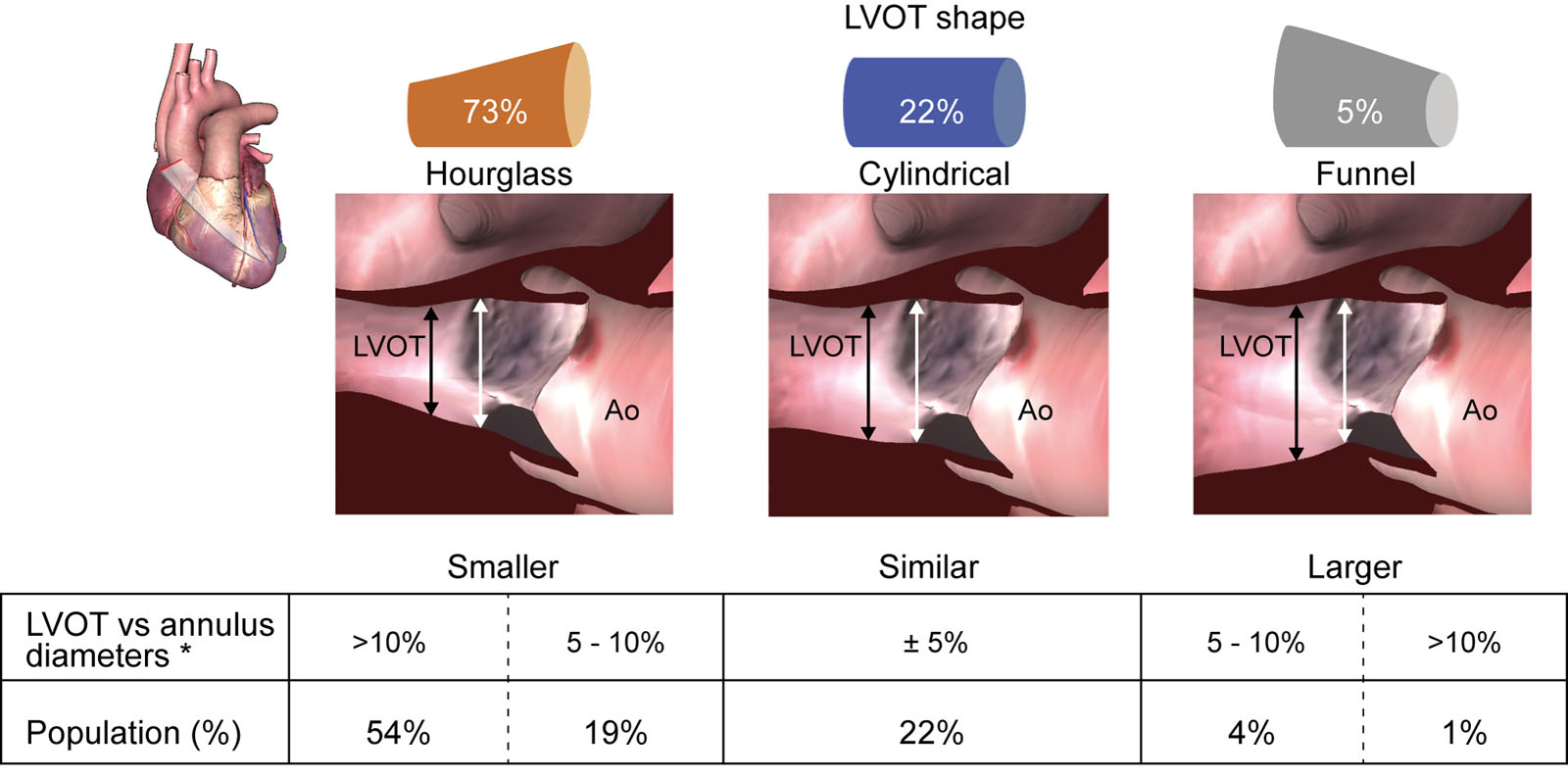
Prevalence of different LVOT shapes and their effect on SV estimation. This figure shows the prevalence of different LVOT shapes in our population along with examples (zoomed ME LAX echocardiographic images). *Bias examples: assuming a theoretical LVOT VTI of 20 cm and an AoV VTI of 80 cm, a 5% error in diameter (e.g., LVOT diameter of 20 mm corresponding to LVOT area 3.14 cm² vs LVOT diameter of 21mm and LVOT area 3.46 cm²) would yield a 10% error in SV (63 vs 69 mL) and AVA (0.79 vs 0.87 cm2). A 10% error in diameter (e.g., LVOT diameter of 20 mm corresponding to LVOT area 3.14 cm2 vs LVOT diameter of 22 mm and LVOT area of 3.80 cm2) would yield a 21% error in SV (63 vs 76 mL) and in AVA (0.79 vs 0.95 cm²). Abbreviations: Ao,aorta; AoV, aortic valve; AVA, aortic valve area; d, diameter; LAX, long-axis; LVOT, left ventricular outflow tract; ME, mid-esophageal; SV, stroke volume; VTI, velocity time integral. Adapted from Guzetti et al.20
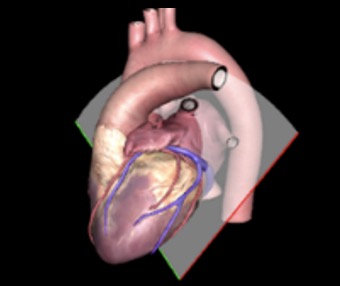
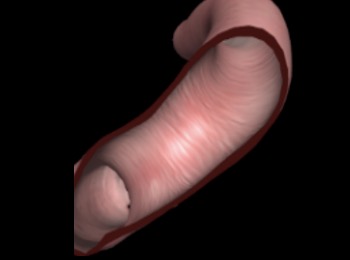
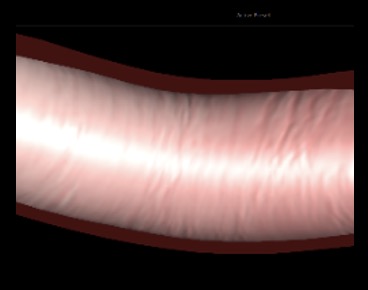
eFigure 14.30
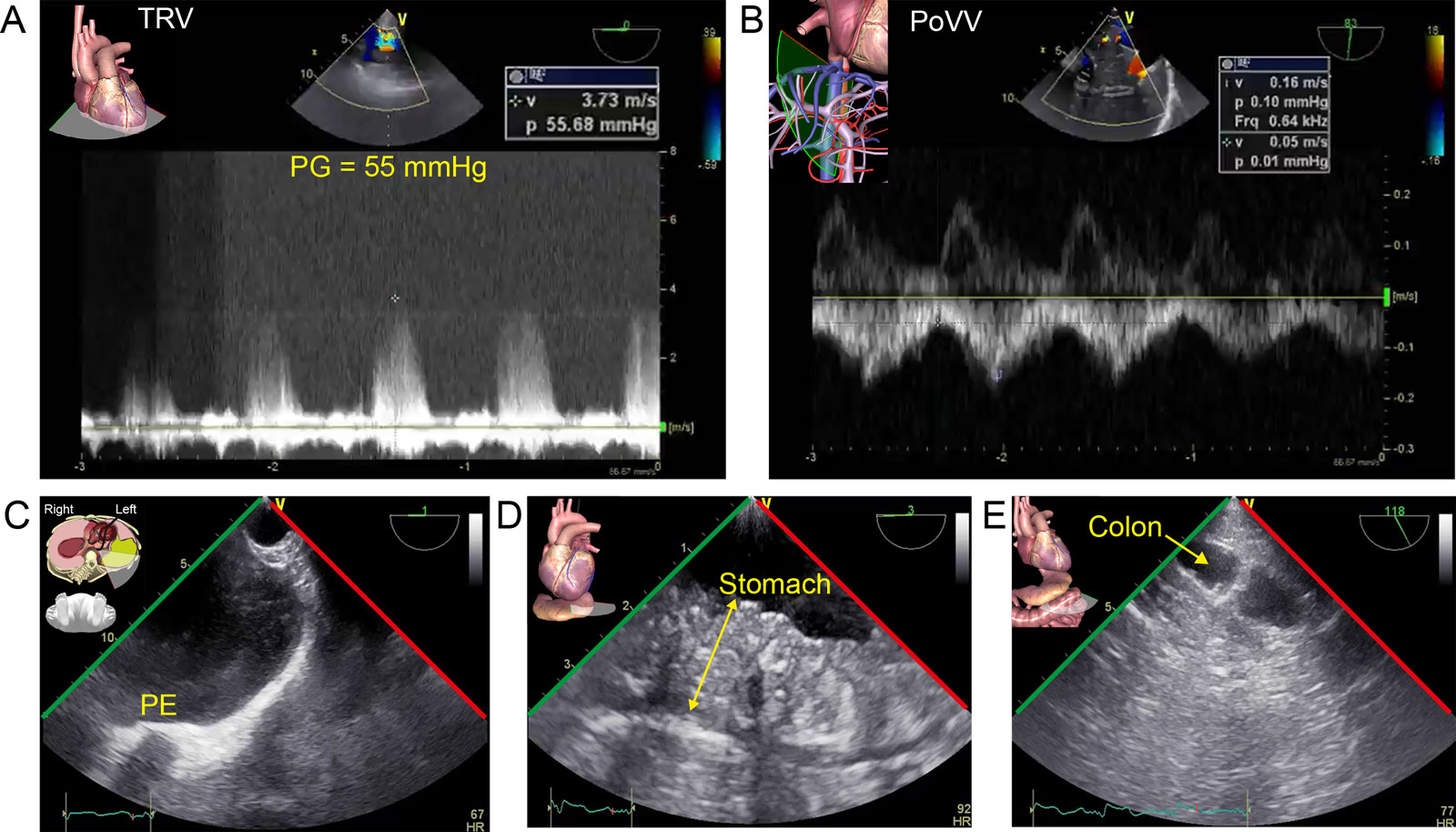
Extra-cardiac AoV stenosis complications. A 79-year-old man with AS presents for THV. (A) CWD interrogation of the TV from the ME RV 4C view shows a TRV peak PG of 55 mmHg. (B) This was associated with portal pulsatility in the PoVV signal. (C-E) TELUS shows a (C) left pleural effusion (PE), and TGAUS shows (D) significant stomach (double arrow) and (E) bowel edema with edema of the semi-lunar fold (arrow). These elements can lead to a cardio-intestinal syndrome.52 Abbreviations: 4C, four- chamber; AoV, aortic valve; CWD, continuous wave Doppler; ME, mid-esophageal; P, pressure; PG, pressure gradient; PoVV, portal vein velocity; RV, right ventricular; TGAUS, transgastric abdominal ultrasound; TELUS, transesophageal lung ultrasound; THV, transcatheter heart valve; TRV, tricuspid regurgitation velocity; TV, tricuspid valve; V, velocity; VV, venous velocity.
eFigure 14.40
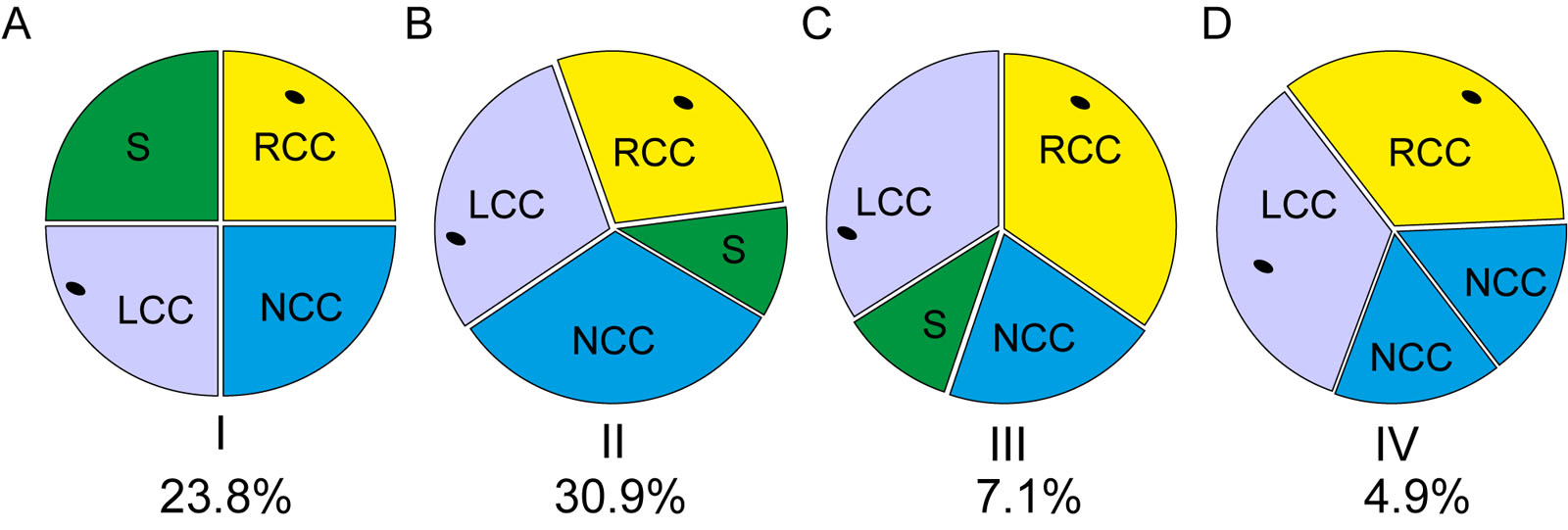
Quadricuspid AoV classification. There are different anatomic classifications that describe the quadricuspid AoV54 including the simplified classification by Nakamura. Abbreviations: AoV, aortic valve; LCC, left coronary cusp; NCC, non-coronary cusp; RCC, right coronary cusp; S, supernumerary cusp. Adapted from Nakamura et al.31
eFigure 14.45
Type II AR. This is an example of AoV RCC prolapse. (A-D) The ME biplane AoV LAX and SAX views with CFI show a RCC partial prolapse with (C, D) a posterior directed AR jet. (E) M-mode of the descending Ao shows increased Ao wall pulsatility (Corrigan pulse). Abbreviations: Ao, aorta; AoV, aortic valve; AR, aortic regurgitation; CFI, color flow imaging; LAX, long-axis; LCC, left coronary cusp; ME, mid-esophageal; NCC, non-coronary cusp; RCC, right coronary cusp; SAX, short-axis.
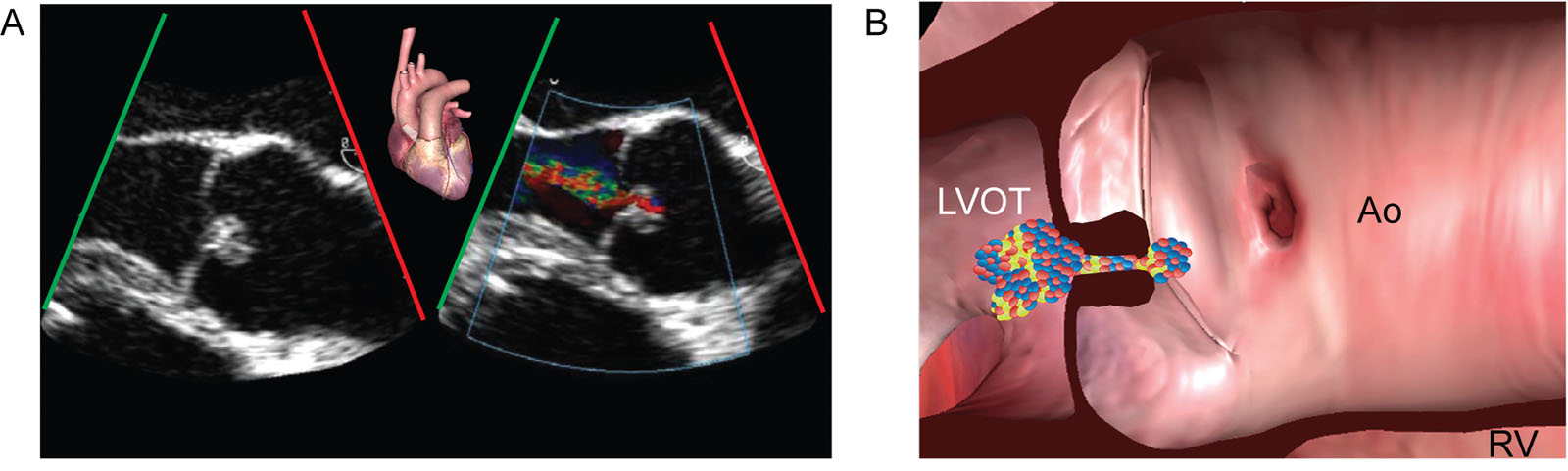
eFigure 14.47
Type III AR. (A, B) The ME AoV LAX view shows thickened cusps that are more echogenic without calcification. There is moderate central AR. Abbreviations: Ao, aorta; AoV, aortic valve; AR, aortic regurgitation; LAX, long-axis; LVOT, left ventricular outflow tract; ME, mid-esophageal; RV, right ventricle.
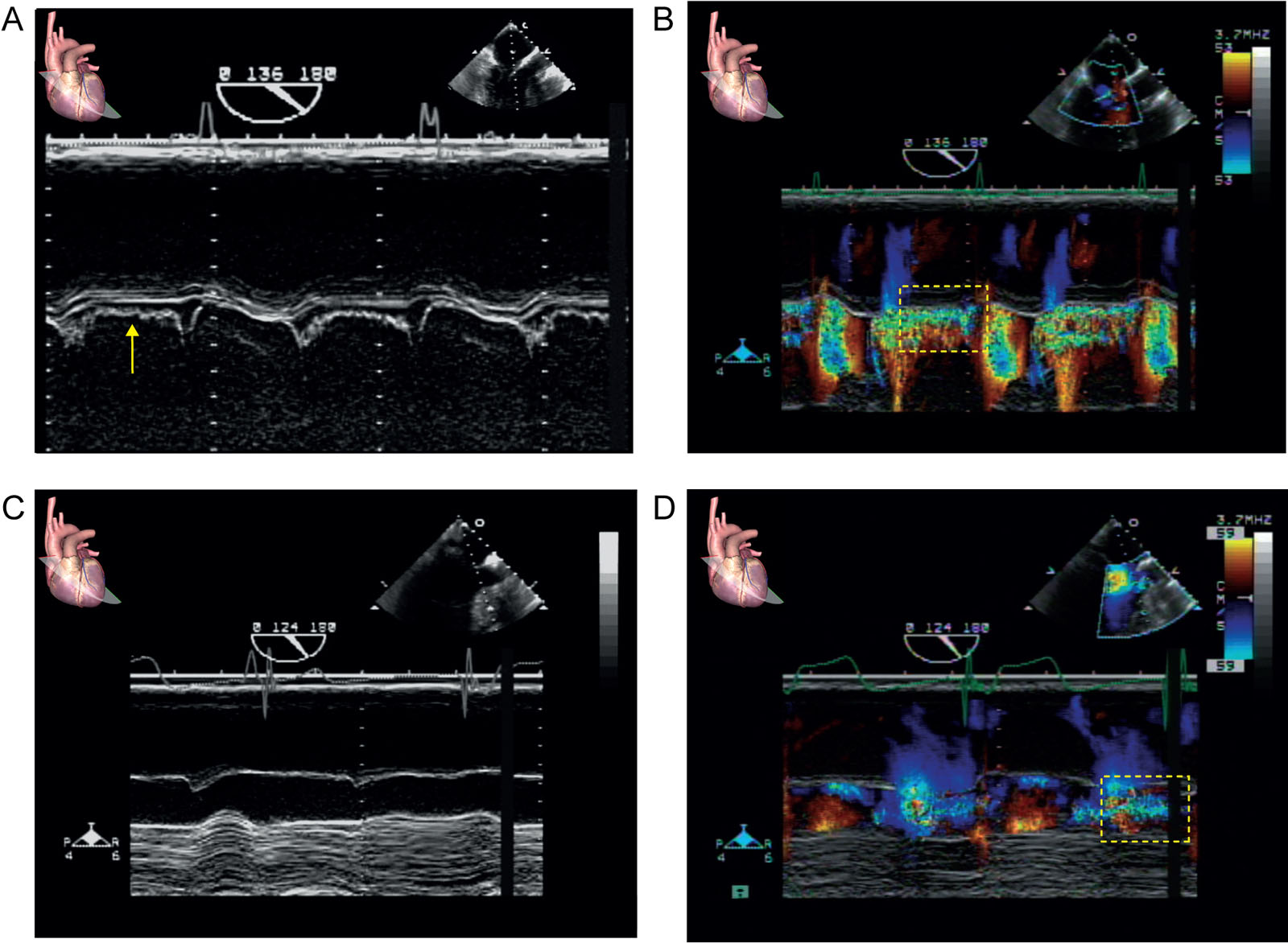
eFigure 14.49
MV fluttering from AR. This is a 56-year-old man with severe AR and AMVL fluttering. M-mode and color M-mode through the AMVL from a ME AoV LAX view (A, B) before and (C, D) after AVR. Note the disappearance of the AMVL fluttering (A, arrow) after intervention. The color M-mode shows significant AR before (box) and (D) trivial AR (box) after AVR. Abbreviations: AMVL, anterior mitral valve leaflet; AoV, aortic valve; AR, aortic regurgitation; AVR, aortic valve replacement; LAX, long-axis; ME, mid-esophageal; MV, mitral valve.
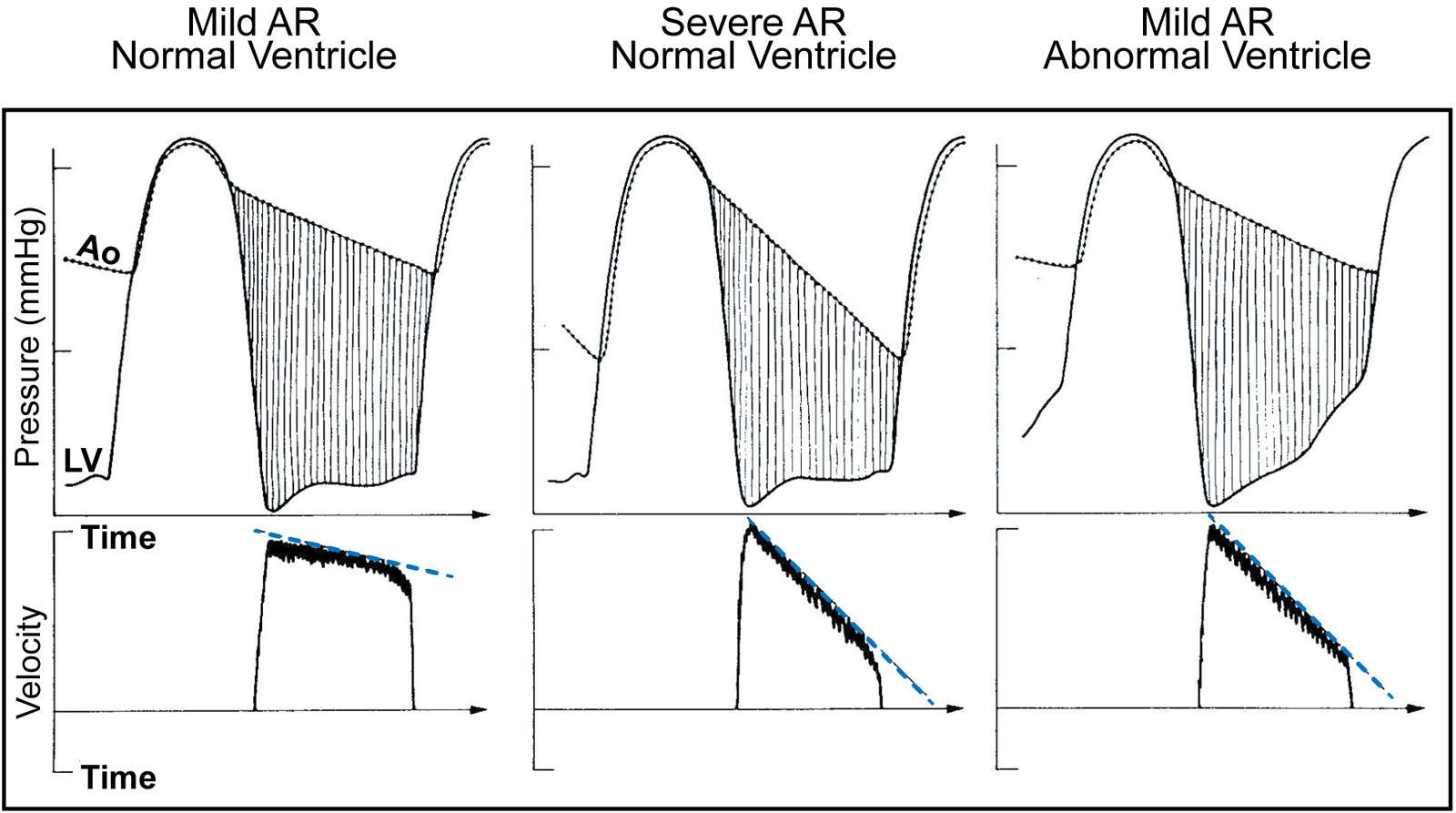
eFigure 14.55
Pressure half-time. This diagram shows the determinants of regurgitant PHT in AR. The upper panels are invasive Ao and LV pressure tracings, the lower panels are CWD tracings across the AoV during diastole. The slope of the blood flow velocity corresponds to the fall in the measured PG between the Ao and LV. Calculation of PHT with Doppler echocardiography derives from the rate of decrease in blood flow velocity across the AoV in patients with AR. Abbreviations: Ao, aorta; AoV, aortic valve; AR, aortic regurgitation; CWD, continuous wave Doppler; LV, left ventricle; PG, pressure gradient; PHT, pressure half-time. Source: Reproduced with permission from Obeid et al.55
Videos
Chapter 14 Fig01C
Chapter 14 Fig02EF
Chapter 14 Fig03
Chapter 14 Fig04A
Chapter 14 Fig04C
Chapter 14 Fig04E
Chapter 14 Fig06A
Chapter 14 Fig06C
Chapter 14 Fig08A
Chapter 14 Fig10B
Chapter 14 Fig12AC
Chapter 14 Fig14D
Chapter 14 Fig15D
Chapter 14 Fig16D
Chapter 14 Fig17AC
Chapter 14 Fig17E
Chapter 14 Fig18A
Chapter 14 Fig18D
Chapter 14 Fig19A
Chapter 14 Fig19C
Chapter 14 Fig20A
Chapter 14 Fig20C
Chapter 14 Fig21A
Chapter 14 Fig21D
Chapter 14 Fig26
Chapter 14 Fig29A
Chapter 14 Fig30C
Chapter 14 Fig30D
Chapter 14 Fig30E
Chapter 14 Fig33A
Chapter 14 Fig33C
Chapter 14 Fig33F
Chapter 14 Fig34A
Chapter 14 Fig34E
Chapter 14 Fig34F
Chapter 14 Fig35A
Chapter 14 Fig35BE
Chapter 14 Fig35D
Chapter 14 Fig35GH
Chapter 14 Fig36D
Chapter 14 Fig36E
Chapter 14 Fig37AD
Chapter 14 Fig37CF
Chapter 14 Fig38A
Chapter 14 Fig38D
Chapter 14 Fig38F
Chapter 14 Fig39A
Chapter 14 Fig39B
Chapter 14 Fig42A
Chapter 14 Fig43A
Chapter 14 Fig43C
Chapter 14 Fig43E
Chapter 14 Fig43F
Chapter 14 Fig44A
Chapter 14 Fig44C
Chapter 14 Fig44EF
Chapter 14 Fig45A
Chapter 14 Fig45C
Chapter 14 Fig45E
Chapter 14 Fig46A
Chapter 14 Fig46C
Chapter 14 Fig47A
Chapter 14 Fig48A
Chapter 14 Fig48C
Chapter 14 Fig50
Chapter 14 Fig52A
Chapter 14 Fig53A
Chapter 14 Fig53B
Tables
eTable 14.1 TEE major views for assessing the AoV
Standard TEE View |
View-Angle-Technique |
Utility |
Disadvantages |
||
|
 |
 |
ME 5C view |
RCC and NCC |
Alignment not optimal with PWD or CWD |
A |
 |
 |
ME AoV SAX |
Easily acquired view |
|
B |
 |
 |
ME AoV LAX Angle: 120-140° |
Good alignment for aortic annular |
Non-circular plane may underestimate AoV annulus diameter |
C |
 |
 |
TG LAX |
Can measure PG across AoV |
Alignment not always best with PWD or CWD |
D |
 |
 |
Deep TG 5C |
Best view to measure AoV PG |
. |
E |
 |
 |
UE Aortic arch LAX |
Useful view to assess AR severity using PWD |
|
F |
 |
 |
Descending aorta LAX |
Parallel alignment can be sub-optimal |
|
Abbreviations: 3D, three-dimensional; 5C, five-chamber; AoV, aortic valve; AR, aortic regurgitation; CFI, color flow imaging; CWD, continuous wave Doppler; LA, left atrium; LAX, long-axis; ME, mid-esophageal; NCC, non-coronary cusp; PG, pressure gradient; PWD, pulsed wave Doppler; RCC, right coronary cusp; SAX, short-axis; TEE, transesophageal echocardiography; TG, transgastric; UE, upper esophageal. Adapted from Hahn et al.48 |
|||||
eTable 14.4 Qualitative and quantitative parameters useful in grading AR severity
| Mild | Moderate | Moderate to severe | Severe | ||
| Structural and qualitative parameters | |||||
| LV size a | Normal | Normal or dilated | Usually dilated | Usually dilated | |
| Aortic leaflets | Normal or abnormal | Normal or abnormal | Abnormal: prolapse, moderate coaptation defect | Abnormal: flail, wide coaptation defect | |
| CFI AR jet width b | Small in central jets | Intermediate | Large: central jet Variable: eccentric jets | Large: central jet Variable: eccentric jets | |
| CFI convergence b | None or small | Intermediate | Intermediate | Large | |
| PWD flow reversal descending aorta c | Proto-diastolic | Intermediate | Holodiastolic EDV 10-19 cm/s | Holodiastolic EDV ≥ 20 cm/s | |
| CWD AR jet density | Incomplete, faint | Dense | Dense | Dense | |
| Semi-quantitative parameters | |||||
| VC width (mm) d | <3 | 3–6 | 3–6 | >6 | |
| Jet width/LVOT diameter (%) b | <25 | 25–45 | 46–64 | >65 | |
| Jet CSA/LVOT CSA (%) b | <5 | 5–20 | 21–59 | >60 | |
| CWD PHT (ms) c | >500 | Intermediate 200-500 | Intermediate 200-500 | Steep <200 | |
| Quantitative parameters | |||||
| EROAR (cm²) d | <0.10 | 0.10–0.19 | 0.20–0.29 | >0.30 | |
| RVol (ml) | <30 | 30–44 | 45–59 | >60 | |
| RF (%) | <30 | 30–39 | 40–49 | >50 | |
| Other modalities | |||||
| CMR RF (%) | <30 | 30–39 | 40–49 | >50 | |
| a Non-significant LV enlargement includes LVEDD < 56mm, LVEDV < 82ml/m², LVESD < 40 mm and LVESV < 30ml/m² b At a Nyquist limit of 50 to 70 cm/s c LV and aortic compliance influence this parameter (See Table 14.5) particularly in the elderly. These parameters are also influenced by chronotropy d 3D echocardiography can evaluate AR mechanism and quantify VC 50, 51, 32 Abbreviations: 3D, three-dimensional; AR, aortic regurgitation; CFI, color flow imaging; CMR, cardiac magnetic resonance; CSA, cross-sectional area; CWD, continuous wave Doppler; EDV, end-diastolic velocity; EROAR, AR effective regurgitant orifice area; LV, left ventricle; LVEDD, left ventricular end-diastolic dimension; LVEDV, left ventricular end-diastolic volume; LVESD, left ventricular end-systolic dimension; LVESV, left ventricular end-systolic volume; LVOT, left ventricular outflow tract; PHT, pressure half-time; PWD, pulsed wave Doppler; RF, regurgitant fraction; RVol, regurgitant volume; VC, vena contracta. Adapted from Zoghbi et al32 and Lancelotti et al.34 | |||||