Figures
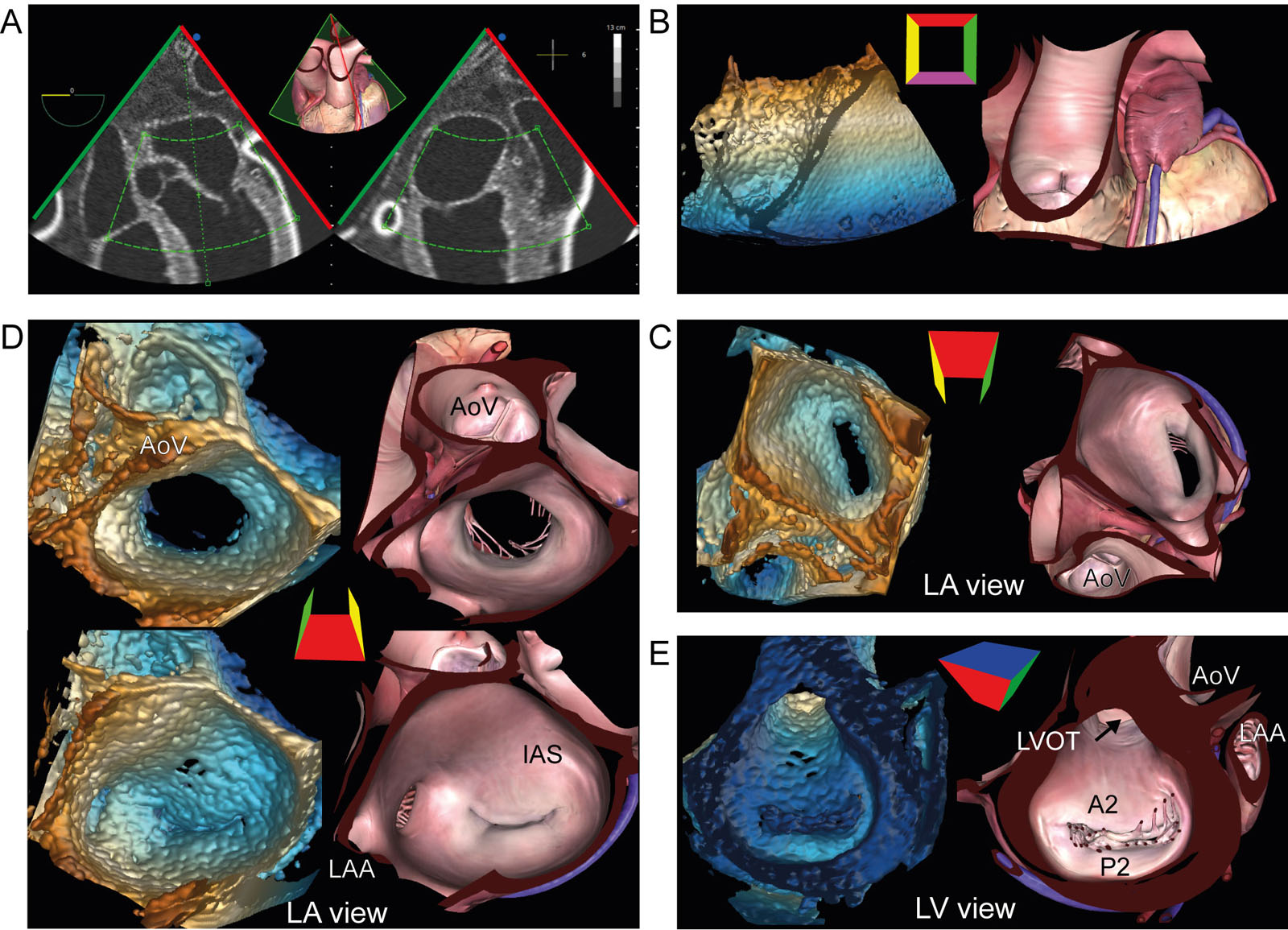
eFigure 16.9
MV 3D zoom acquisition. (A) 3D zoom acquisition should include both MV leaflets, the mitral annulus, and part of the AoV. (B) After acquisition, the 3D frustum is rotated (C) downwards to show the MV from the LA perspective with (D) Z-rotation to position the AoV at the top (12 o’clock) of the display in diastole and in systole. (E) Rotating the 3D frustum 180° from the LA perspective shows the LV perspective. Abbreviations: 3D, three-dimensional, AoV, aortic valve; IAS, interatrial septum; LA, left atrium; LAA, left atrial appendage; LV, left ventricle; LVOT, left ventricular outflow tract; MV, mitral valve.
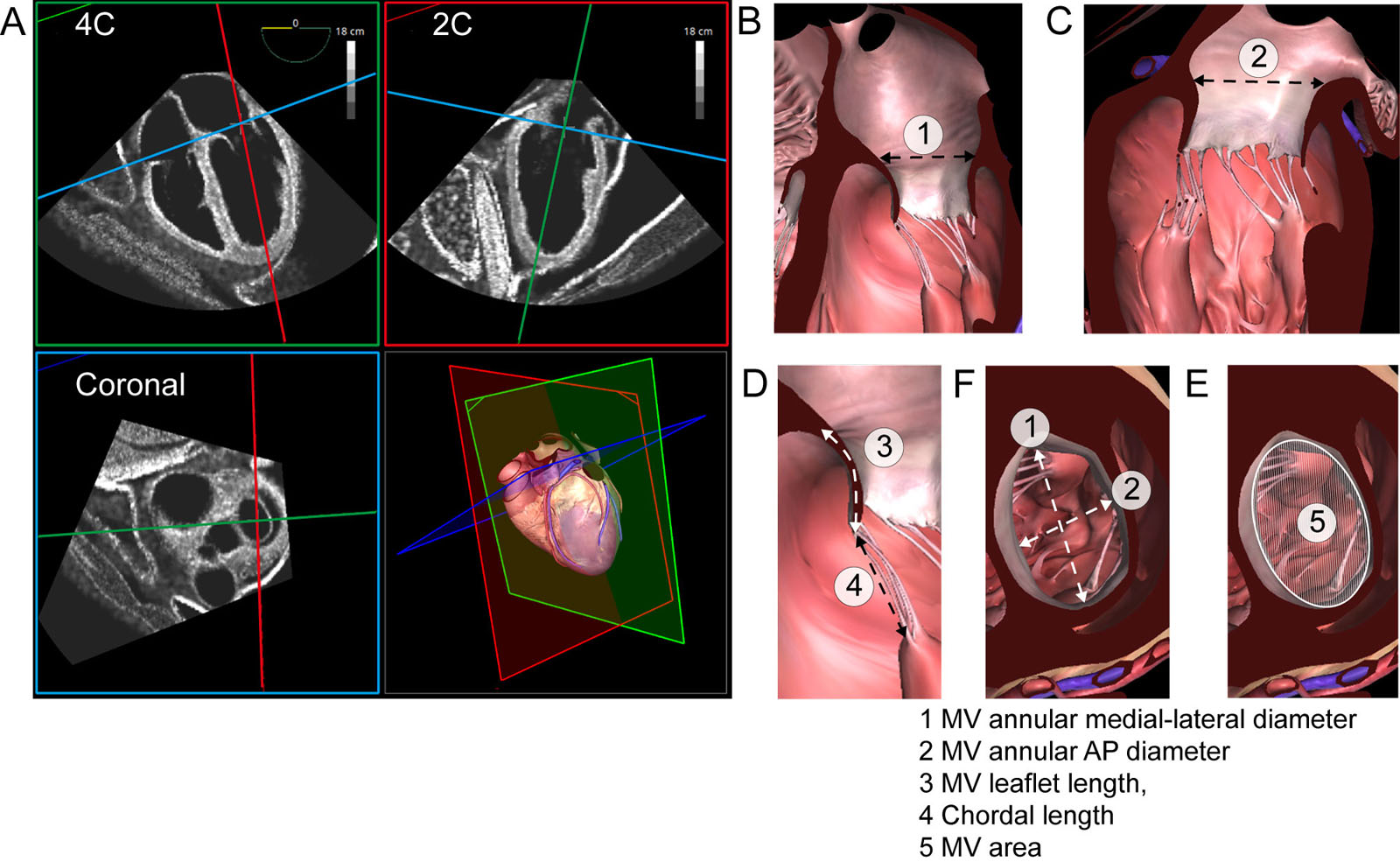
eFigure 16.10
MV MPR measurements. (A) Mid diastolic MV measurements of the mitral annulus dimensions from a simulated 3D TEE dataset showing the ME 4C, orthogonal ME 2C view and coronal view through the TV and MV annuli. (B-F) The derived measurements include: 1) MV annular medial-lateral diameter, 2) MV annular AP diameter, 3) MV leaflet length, 4) chordal length, and 5) MV area. Abbreviations: 2C, two-chamber; 3D, three-dimensional; 4C, four-chamber; AP, antero-posterior; ME, mid-esophageal; MPR, multiplane reconstruction; MV, mitral valve; TEE transesophageal echocardiography; TV, tricuspid valve.
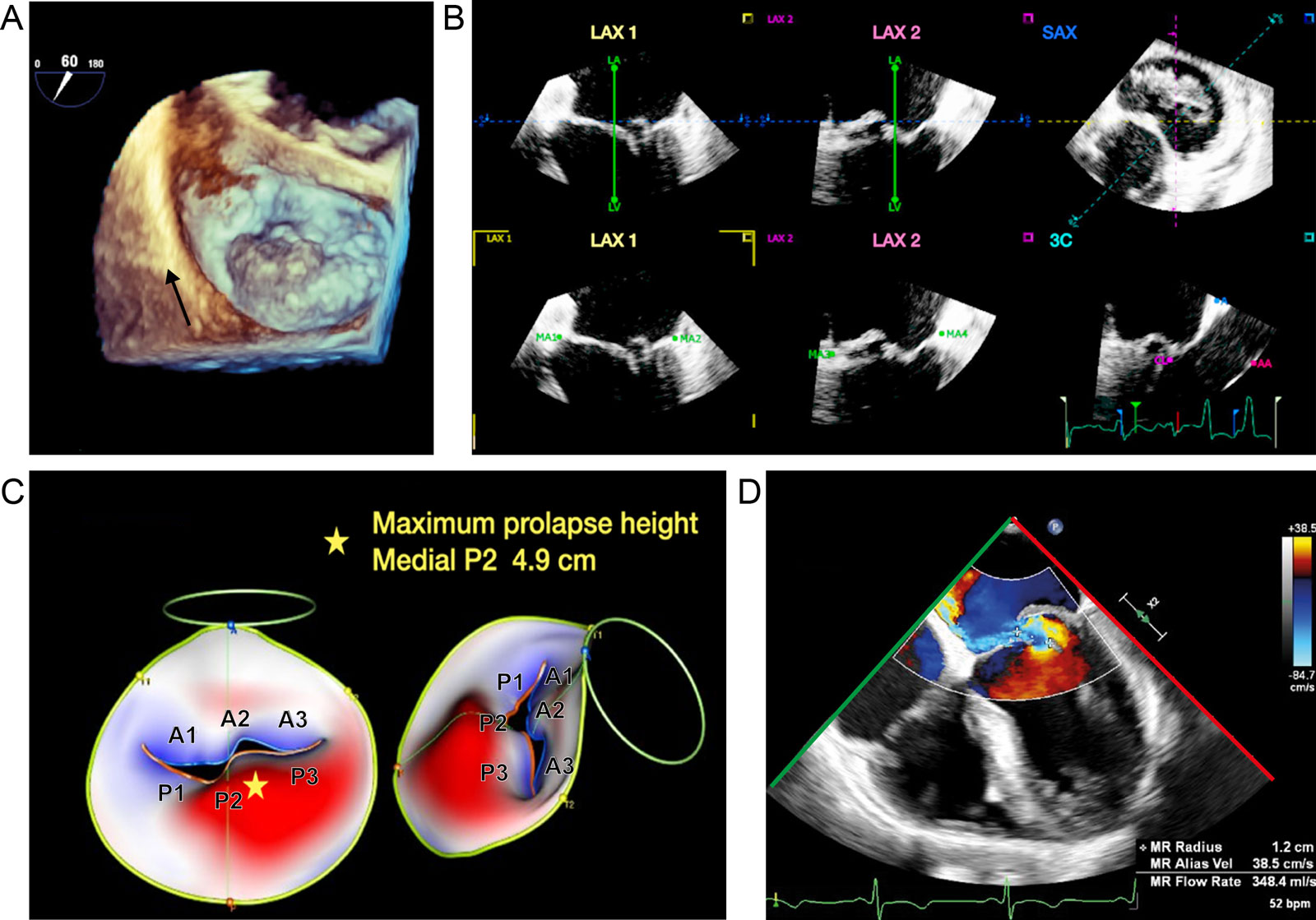
eFigure 16.12
Dynamic 3D parametric MV model. (A) This is a 3D “en-face” view of the MV, in a patient with MV prolapse and flail. (B) This semi-automated software allows the user to align and landmark the 3D MV dataset in MPR views. (C) Subsequent analysis produces a dynamic systolic parametric MV model, showing P2 flail and P3 prolapse from “en-face” and side perspectives. Analysis gives the maximal MV prolapse height, which corresponds to the flail medial P2 segment. Sophisticated 3D measurements as annular diameters, annular non-planarity, commissural lengths, leaflet dimensions, and aortic to mitral annular orientation are possible. (D) ME 4C with CFI demonstrates an eccentric anterior directed MR jet resulting from P2 flail. Abbreviations: 3C, three-chamber; 3D, three-dimensional; 4C. four-chamber; CFI, color flow imaging; LAX, long-axis; ME, mid-esophageal; MPR, multiplane reconstruction; MR, mitral regurgitation; MV, mitral valve; P, posterior; SAX; short-axis.
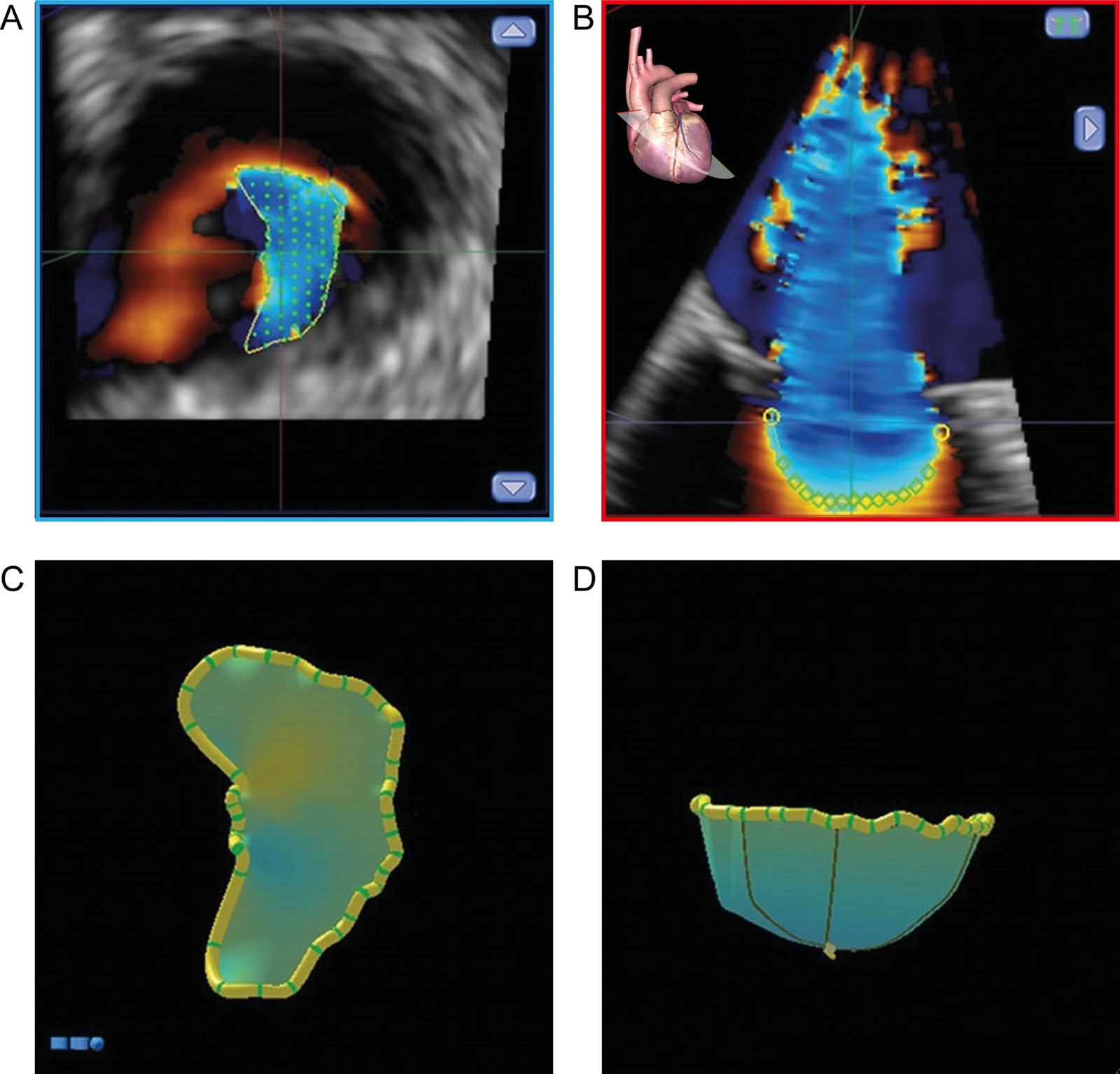
eFigure 16.29
3D PISA. This represents computer-assisted 3D PISA shell reconstruction from a 3D TEE CFI dataset. (A) SAX view of the crescent-shaped PISA base. (B) ME LAX view with PISA (C) SAX view of the reconstructed, CFI 3D-rendered surface representing a topographical map of the PISA. (D) LAX view of the reconstructed, color-coded, 3D-rendered surface representing a topographical map of the PISA. Abbreviations: 3D, three-dimensional; CFI, color flow imaging; LAX, long-axis; ME, mid-esophageal; PISA, proximal isovelocity surface area; SAX, short-axis; TEE, transesophageal echocardiography. Adapted from Ashikhmina et al.46
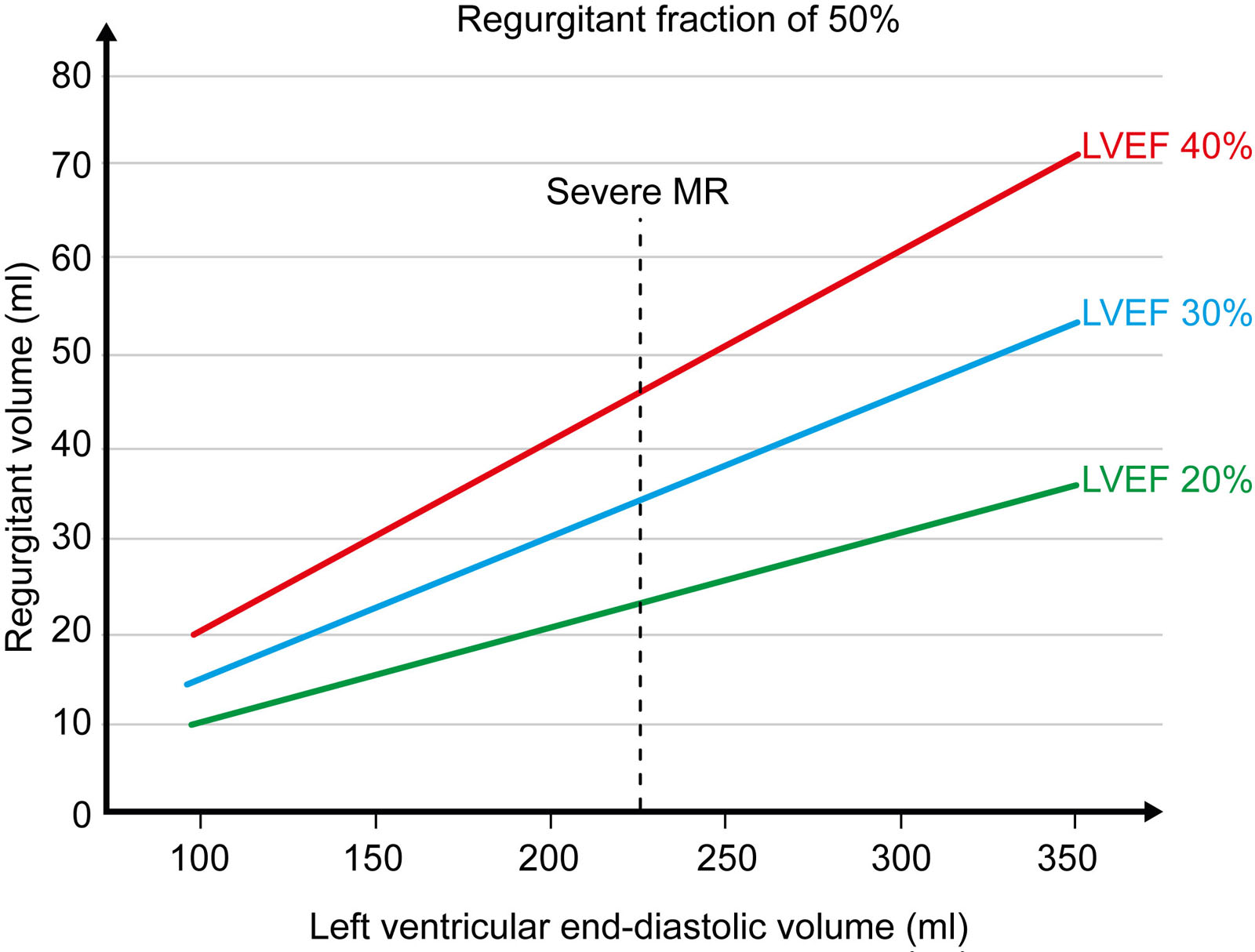
eFigure 16.32
RVol and LVEF. This graph shows the variations in MV RVol versus LV end-diastolic volume at different LVEFs. The RVol changes with LVEF and never exceeds 60 ml in patients with LVEF < 30%. The RVol may exceed 60 ml in patients with LVEF > 40% only in very dilated LV (LVEDV > 300 ml). At normal LV size, RVol can be below 30 ml, even when RF is 50%. With an LVEDV of 230 ml (dotted vertical line; mean for heart failure clinical trials), severe MR by RF criteria occurs at 45 ml for an LVEF of 40%, 35 ml for LVEF 30%, and <25 ml for LVEF 20%. Abbreviations: LV, left ventricle; LVEDV, left ventricular end-diastolic volume; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; MV, mitral valve; RF, regurgitant fraction; RVol, regurgitant volume. Adapted from Grayburn et al.49
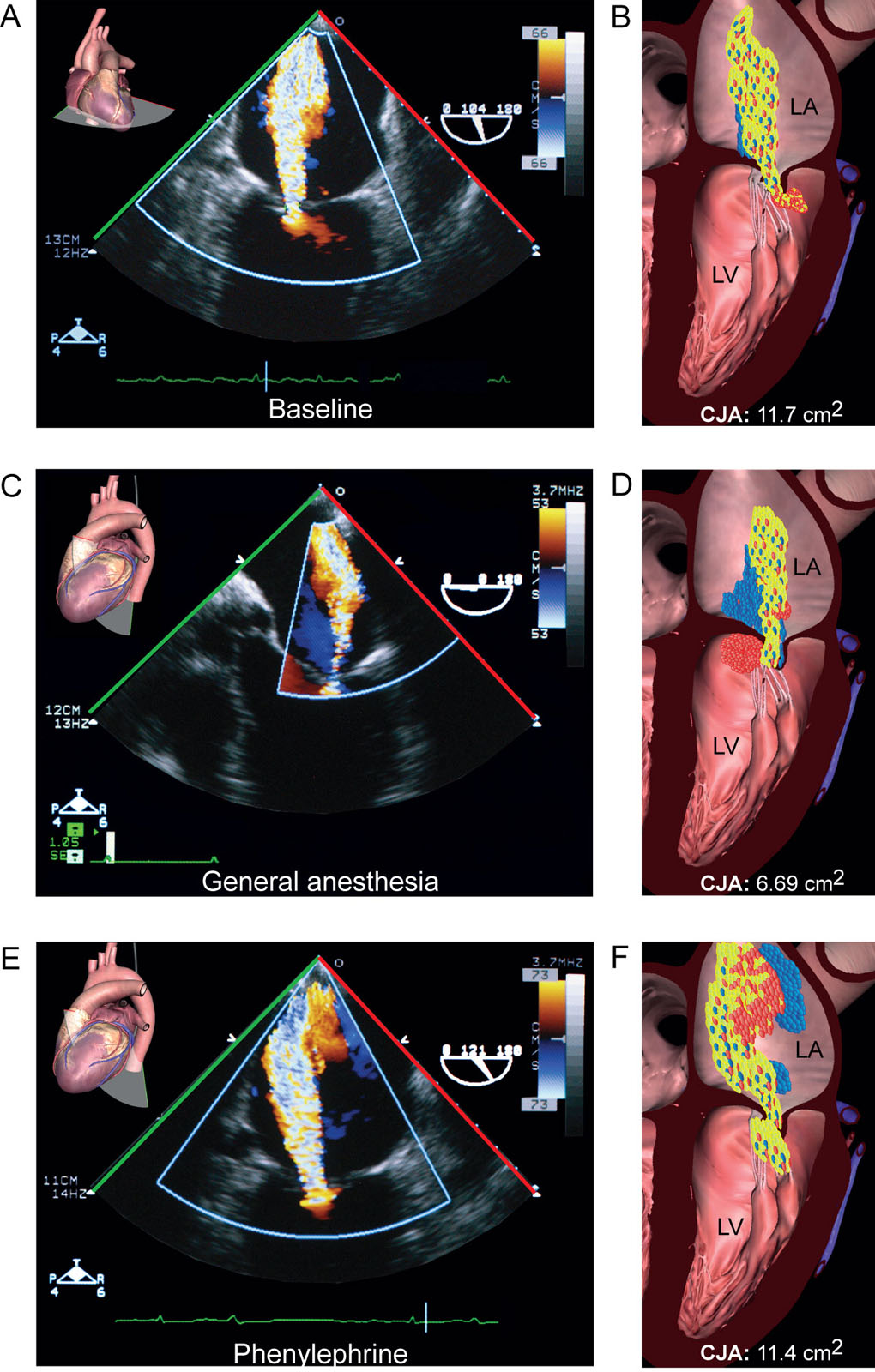
eFigure 16.33
CFI jet area and general anesthesia. CFI jet areas appear from different ME views in a patient with MR during (A,B) awake baseline state. (C,D) after induction of general anesthesia and (E, F) using phenylephrine to obtain the same systolic arterial pressure (150 mmHg) as during baseline. Note the reduced CFI jet area during general anesthesia. Abbreviations: CFI, color flow imaging; CJA, color jet area; LA, left atrium; LV, left ventricle; ME, mid-esophageal; MR, mitral regurgitation. Adapted from Gisbert et al.41
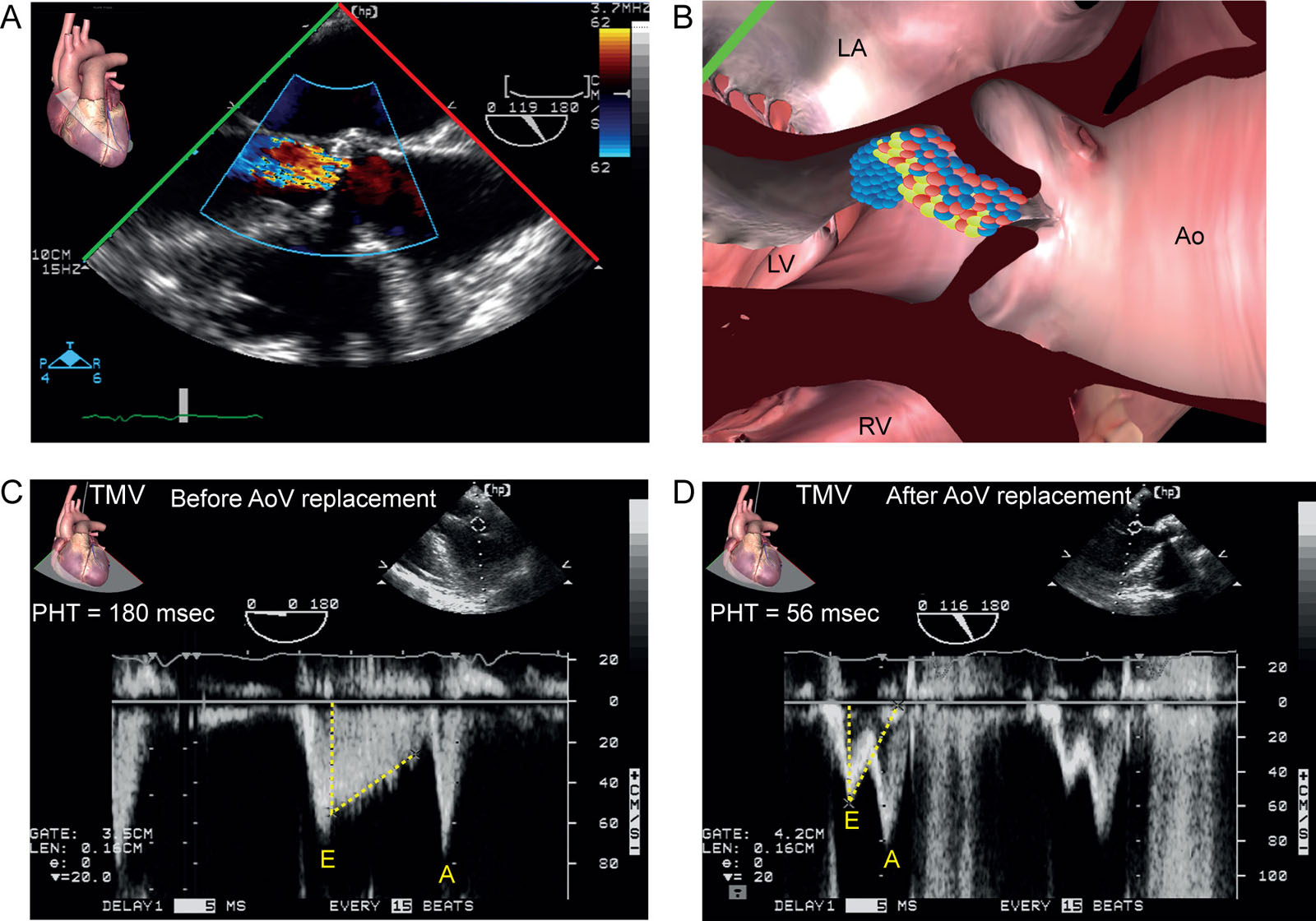
eFigure 16.39
Pseudo MV stenosis. (A, B) ME AoV LAX view with CFI view in a 78-year-old woman scheduled for AoV replacement. (C) The AoV regurgitation was associated with a pseudo MS CWD pattern from either restricted opening of the MVAL or contamination from the AoV regurgitation signal. The PHT obtained from the Doppler TMV was 180 ms compared with (D) 56 ms after AVR. Abbreviations: A, peak late diastolic TMV; Ao, aorta; AoV, aortic valve; AVR, aortic valve replacement; CFI, color flow imaging; CWD, continuous wave Doppler; E, peak early diastolic TMV; LA, left atrium; LAX, long-axis; LV, left ventricle; ME, mid-esophageal; MS, mitral stenosis; MS, mitral stenosis; MV, mitral valve; MVAL, mitral valve anterior leaflet; PHT, pressure half-time; RV, right ventricle; TMV, transmitral velocity.
Videos
Chapter 16 Fig01
Chapter 16 Fig04C
Chapter 16 Fig04D
Chapter 16 Fig05B
Chapter 16 Fig05D
Chapter 16 Fig05F
Chapter 16 Fig05H
Chapter 16 Fig06B
Chapter 16 Fig06D
Chapter 16 Fig06F
Chapter 16 Fig06H
Chapter 16 Fig07A
Chapter 16 Fig07D
Chapter 16 Fig07G
Chapter 16 Fig08A
Chapter 16 Fig08B
Chapter 16 Fig09
Chapter 16 Fig12C
Chapter 16 Fig12D
Chapter 16 Fig13B
Chapter 16 Fig14A
Chapter 16 Fig14B
Chapter 16 Fig14C
Chapter 16 Fig16A
Chapter 16 Fig16B
Chapter 16 Fig16D
Chapter 16 Fig16E
Chapter 16 Fig17A
Chapter 16 Fig17B
Chapter 16 Fig17D
Chapter 16 Fig17E
Chapter 16 Fig18A
Chapter 16 Fig18B
Chapter 16 Fig18E
Chapter 16 Fig18F
Chapter 16 Fig19A
Chapter 16 Fig19B
Chapter 16 Fig19D
Chapter 16 Fig19E
Chapter 16 Fig19F
Chapter 16 Fig20A
Chapter 16 Fig20C
Chapter 16 Fig20D
Chapter 16 Fig20E
Chapter 16 Fig21A
Chapter 16 Fig21B
Chapter 16 Fig21D
Chapter 16 Fig21E
Chapter 16 Fig22A
Chapter 16 Fig22C
Chapter 16 Fig22D
Chapter 16 Fig23A
Chapter 16 Fig23C
Chapter 16 Fig23E
Chapter 16 Fig24A
Chapter 16 Fig28A
Chapter 16 Fig28D
Chapter 16 Fig35FG
Chapter 16 Fig35H
Chapter 16 Fig36A
Chapter 16 Fig36C
Chapter 16 Fig36E
Chapter 16 Fig36F
Chapter 16 Fig37AE
Chapter 16 Fig39A
Tables
eTable 16.2 Grading chronic MR severity by echocardiography
| MR severity classes a | Mild | Mild-to-moderate | Moderate-to-severe | Severe | |
| MR severity sub-classesj | (Grade 1 or 1+) | (Grade 2 or 2+) | (Grade 3 or 3+) | (Grade 4 or 4+) | |
| Structural and qualitative parameters | |||||
| LV and LA size b | Usually normal | Normal or dilated | Usually dilated | Usually dilated | |
| PA [DB1] pressures b | Usually normal | Normal or elevated | Normal or elevated | Usually elevated | |
| MV morphology | None or mild leaflet abnormality or minimal tenting | Moderate leaflet abnormality or moderate tenting | Moderate leaflet abnormality or moderate tenting | Flail leaflet/large coaptation defect/severe tenting | |
| CFI MR jet area c | Small, central <4 cm² or < 20% of LA area | Intermediate 4-6 cm² or 20-30% of LA area | Intermediate 6-8 cm² or 30-40% of LA area | Large central jet (usually > 8 cm² or > 50% of LA area) or eccentric jet swirling reaching posterior LA wall | |
| CFI convergence zone d | Not visible | Transient or small | Intermediate in size and duration | Large throughout systole | |
| CWD signal of MR jet | No or small faint/parabolic | Dense, partial or parabolic | Dense, parabolic or triangular | Holosystolic/dense/triangular | |
| Semi-quantitative parameters | |||||
| VC width (mm) | < 3 | 3 to < 5 | 5 to < 7 | ≥ 7 (≥8 for biplane)e | |
| PVV with PWD | Systolic dominance f | Normal or systolic blunting g | Systolic blunting g | Minimal to no systolic flow/systolic flow reversalg | |
| TMV with PWD | A-wave dominantb | Variable | E-wave dominant (Peak E > 1.2 m/s)f | E-wave dominant (Peak E > 1.2 m/s)f | |
| MAVIR | < 1 | Intermediate | > 1.2h | > 1.4h | |
| Quantitative Parametersi,jk | |||||
| EROAMR (mm²) | < 20 | 20 - 29 | 30 – 39 | ≥ 40 | |
| RVol (ml)l | < 30 | 30 - 44 | 45 – 59 | ≥ 60 | |
| RF (%) | < 30 | 30 - 39 | 40 – 59 | ≥ 50 | |
| aAll parameters have limitations, so use an integrated approach that weighs the strength of each echocardiographic measurement. Interpret all findings in an individualized manner that accounts for body size, sex, and all patient characteristics. b Mostly for primary MR. Unless, for other reasons, the LA and LV size and the pulmonary pressure are usually normal in patients with mild MR. In acute severe MR, the pulmonary pressures are usually elevated while the LV size is still often normal. In chronic severe MR, the LV classically dilates. Accepted cut-off values for non-significant left-sided chambers enlargement: LA volume <36 mL/m2, LVEDD <56 mm, LVEDV <82 mL/m2, LVESV <40 mm, LVESV <30 mL/m2, LA diameter <39 mm, LA volume <29 mL/m2. LV and LA can be within the ‘‘normal’’ range for patients with acute severe MR or with chronic severe MR who have small body size, particularly women, or with small LV size preceding the occurrence of MR. c At a Nyquist limit of 50 to 70 cm/s. d Convergence is usually < 0.3 cm, and large is ≥ 1 cm at a Nyquist limit of 30-40 cm/sec. e For average between ME 4C and ME 2C. f After 50 year-old. Influenced by many other factors (LV diastolic function, atrial fibrillation, LA pressure). g Unless other reasons for systolic blunting (LV diastolic function, atrial fibrillation, LA pressure). h In the absence of elevated LA pressure or mitral stenosis. MAVIR > 1 is typically associated with severe MR60 I The measurement of the PISA by 2D TTE in patients with secondary MR may underestimate the true ERO because of the crescentic shape of the proximal convergence. j Grading of severity of MR classifies regurgitation as mild, moderate or severe, and sub-classifies the moderate group into ‘mild-to-moderate’ and ‘moderate-to-severe’. In secondary MR, an EROA >30 mm2 and/or a R Vol >45[DB2] mL can define severe MR. k Discrepancies between EROA, RVol, and RF may occur with low or high flow states. l MR regurgitant volume may be lower in low flow conditions but corresponds to a larger RF | |||||
| Abbreviations: 2C, two-chamber; 4C, four-chamber; 2D, two-dimensional; A, late filling TMV; CFI, color flow imaging; CWD, continuous wave Doppler; D, diastolic PVV; E, early filling TMV; ERO, effective regurgitant orifice; EROAMR, effective regurgitant orifice area; LA, left atrium; LV, left ventricle; LVEDD, left ventricular end-diastolic dimension; LVEDV, left ventricular end-diastolic volume; LVESD, left ventricular end-systolic dimension; LVESV, left ventricular end-systolic volume; MAVIR, mitral-aortic flow velocity integral ratio (VTI mitral/VTI LVOT); ME, mid-esophageal; MR, mitral regurgitation; MV, mitral valve; Pa, pulmonary; PISA, proximal isovelocity surface area; PVV, pulmonary venous velocity; PWD, pulsed wave Doppler; RF, regurgitant fraction; RVol, regurgitant volume; TMV, transmitral velocity; TTE, transthoracic echocardiography; VC, vena contracta; VTI, velocity time integral. Adapted from Zoghbi 4 and Lancelotti et al. 3 | |||||