Figures
eFigure 17.7
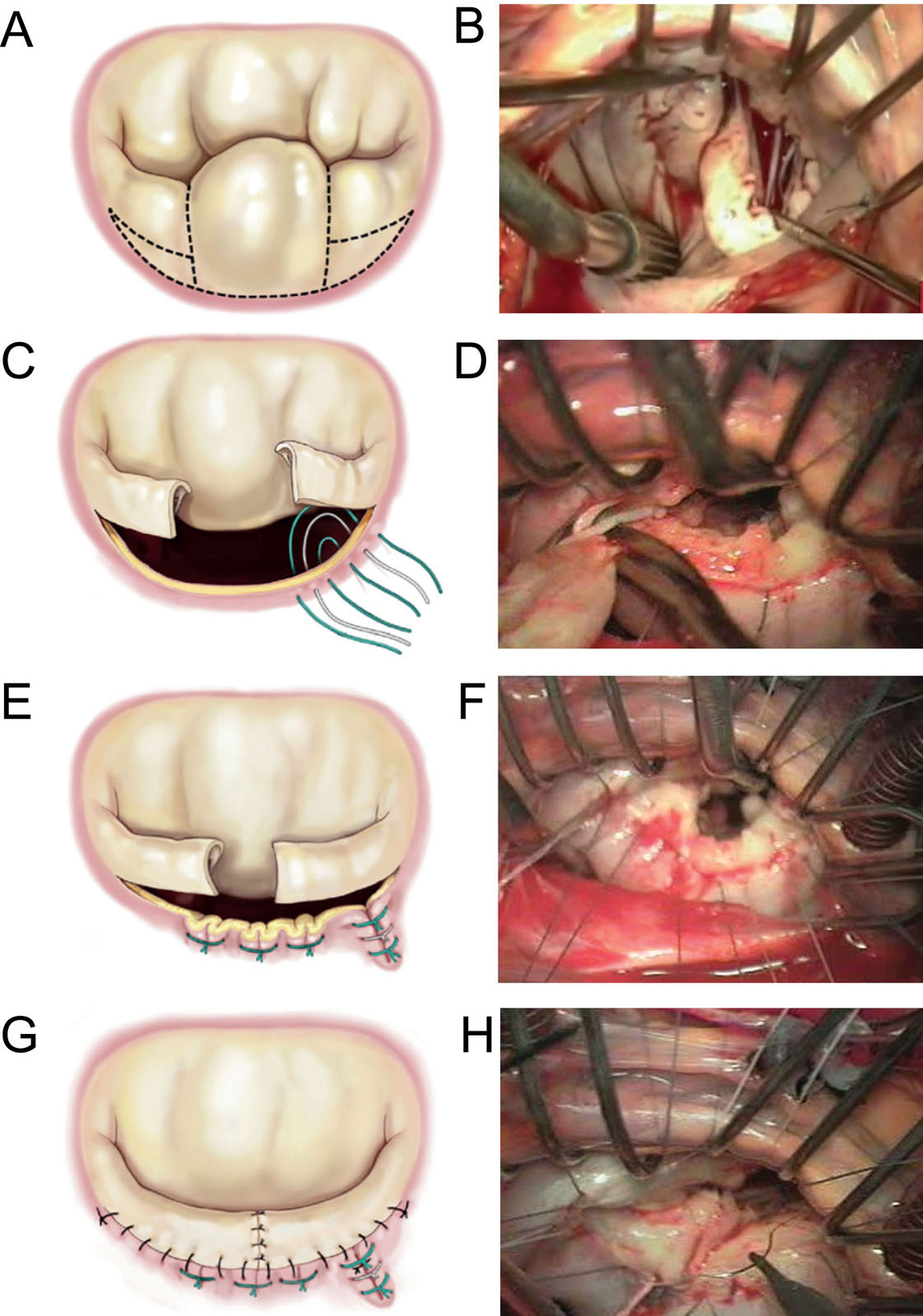
MV repair in Barlow’s disease. These diagrams and intraoperative photos show a complex MV repair of (A, B) P2 prolapse that includes the (C, D) resection line for quadrangular resection and leaflet sliding plasty, (E, F) vertical compression and the (G, H) completed suture lines. Abbreviation: MV, mitral valve. Adapted from Chikwe et al. 18Photos courtesy of Dr. Michel Pellerin.
eFigure 17.8
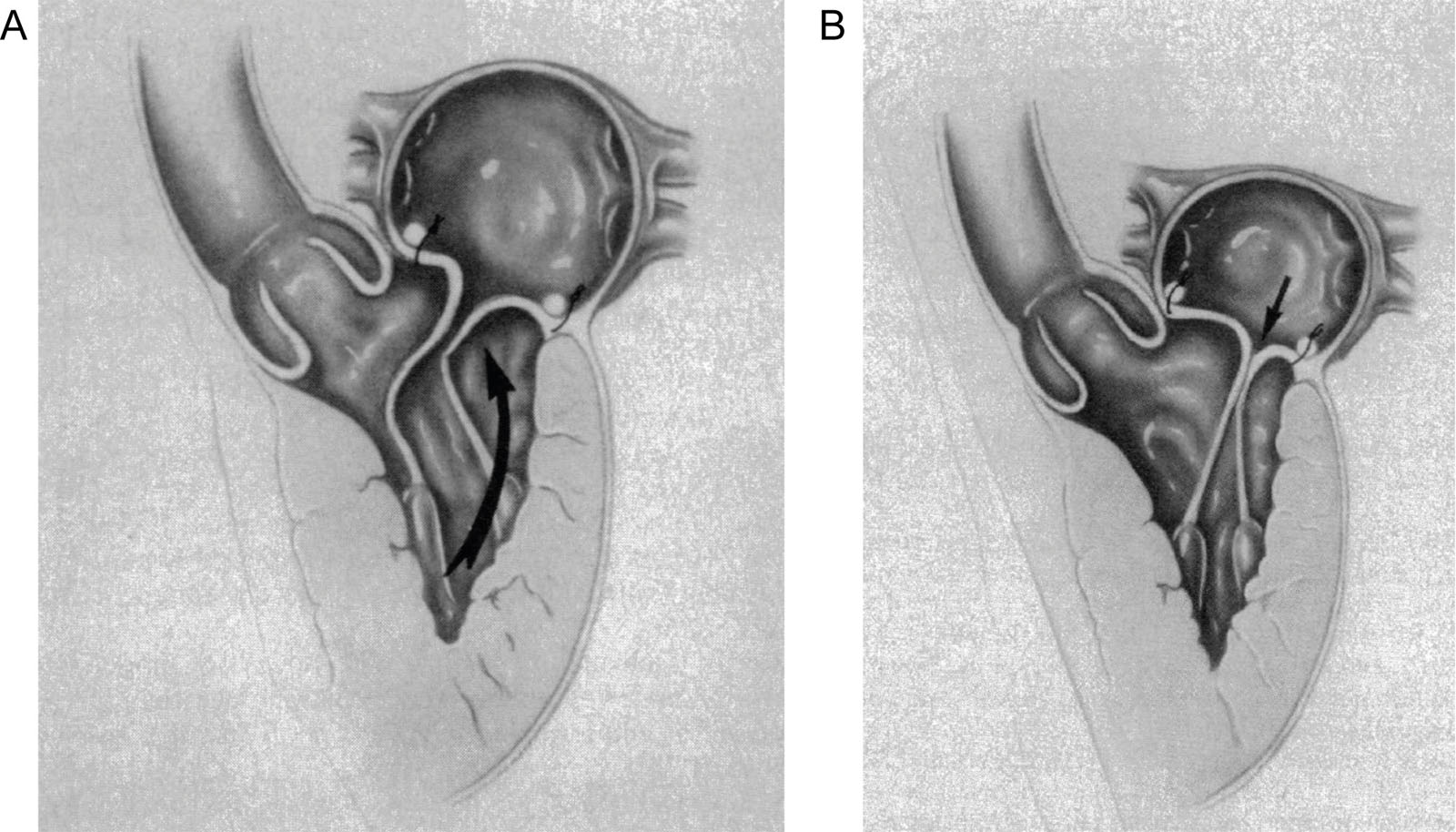
Sliding technique. (A) An inadequate repair will result in LV flow closing the posterior leaflet, which pushes the anterior leaflet toward the LVOT. (B) The sliding leaflet technique reduces the posterior leaflet height so the anterior leaflet closes away from the LVOT. Abbreviation: LV, left ventricle; LVOT, left ventricular outflow tract. With permission from Jebara et al.19
eFigure 17.9
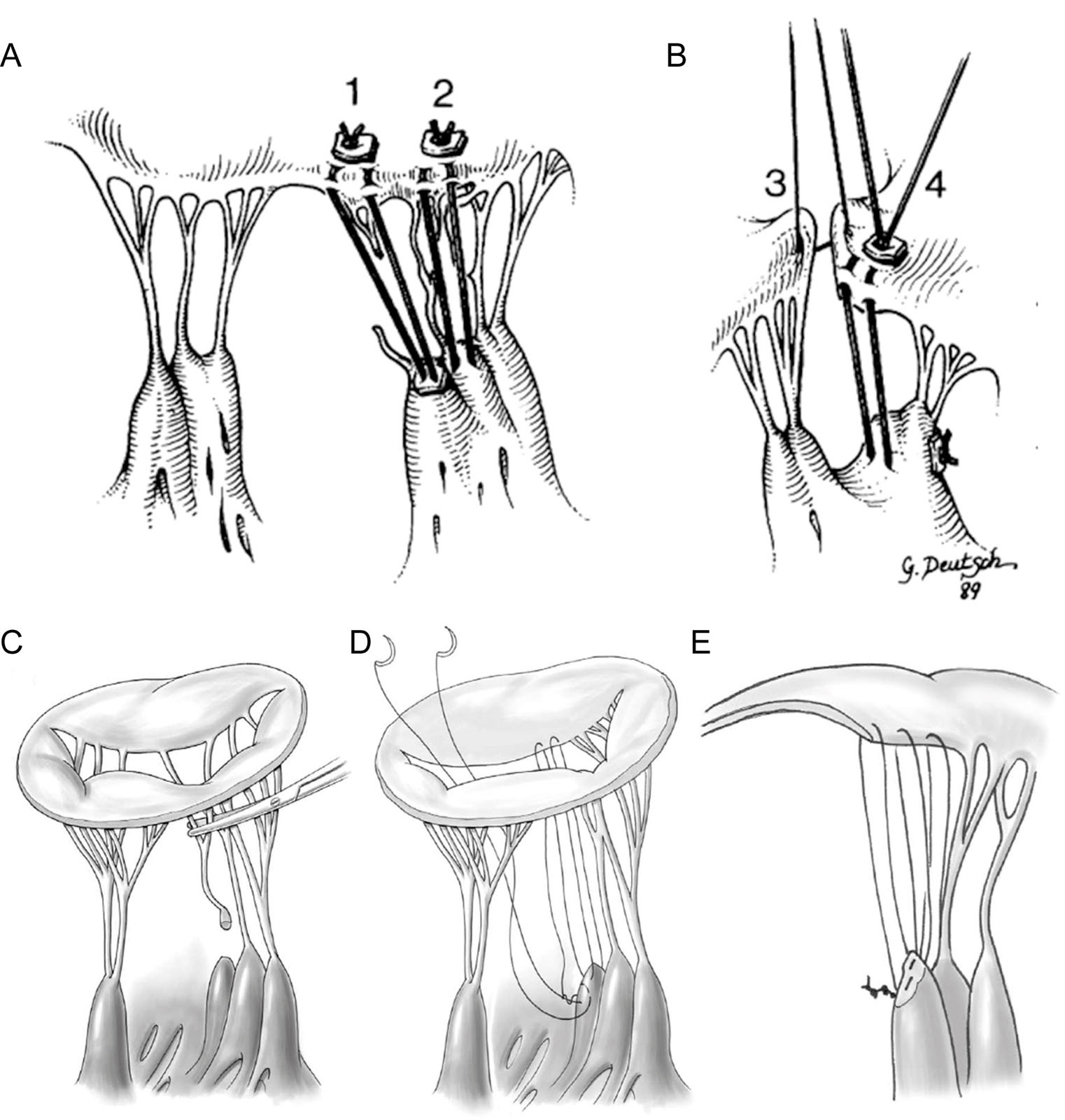
Chordal repair techniques. (A) Replacement for anterior chordae rupture and elongation. (#1), replacement of the ruptured main chorda to medial side of anterior cusp. Extruded PTFE suture is tied at the papillary level on a pledget. At the cusp, the suture has been passed through the thickened free edge and tied over a piece of autogenous pericardium; (#2), attenuated, elongated, paramedial chordae have been judged too thin for shortening. Furthermore, the papillary muscle is sessile. Another pair of new chordae function for these. An alternative papillary technique with a pledget on one side only is used. (B) Length is adjusted so that opposing free edges are parallel with the chordae under tension. (#3), a temporary suture is pulled to keep the chordae taut while the chordae are tied (#4). (C-E) Operative technique to replace ruptured chordae tendineae with Gore-Tex sutures. A single suture is successively passed through the papillary muscle and free margin of the leaflet to create several pairs of artificial chordae. Abbreviations: PTFE, polytetrafluorethylene. Adapted from Frater 20 and David 21.
eFigure 17.12
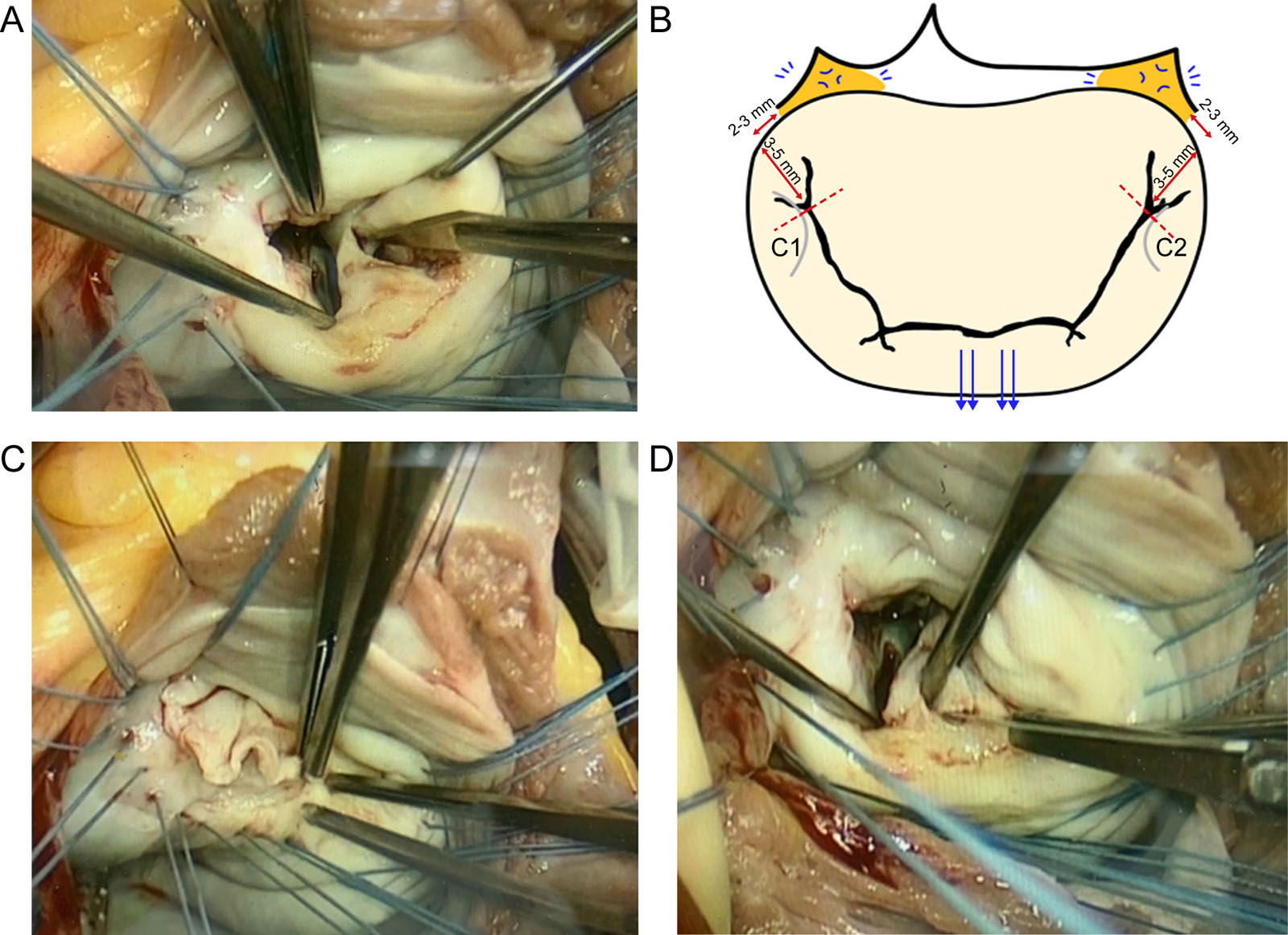
Rheumatic valvular disease repairs. (A) Intraoperative antero-lateral commissurotomy being performed. (B) Schematic illustration of how commissurotomy is performed in Bristol, UK. The blue arrows depict symmetrical traction on the AMVL perpendicular to the inter-trigonal line, which creates dimpling, depicted by the blue markings, subsequently identifying the trigones (orange zones). Red dotted line: ideal point up to which commissurotomy should be performed, stopping 3-5 mm from the annulus and 2-3 mm laterally from the trigone (red bars). (C) Leaflet peeling and (D) posterior mitral leaflet fenestration and chordal resection. Abbreviation: AMVL, anterior mitral valve leaflet. Adapted from Dejsupa et al.27
eFigure 17.13
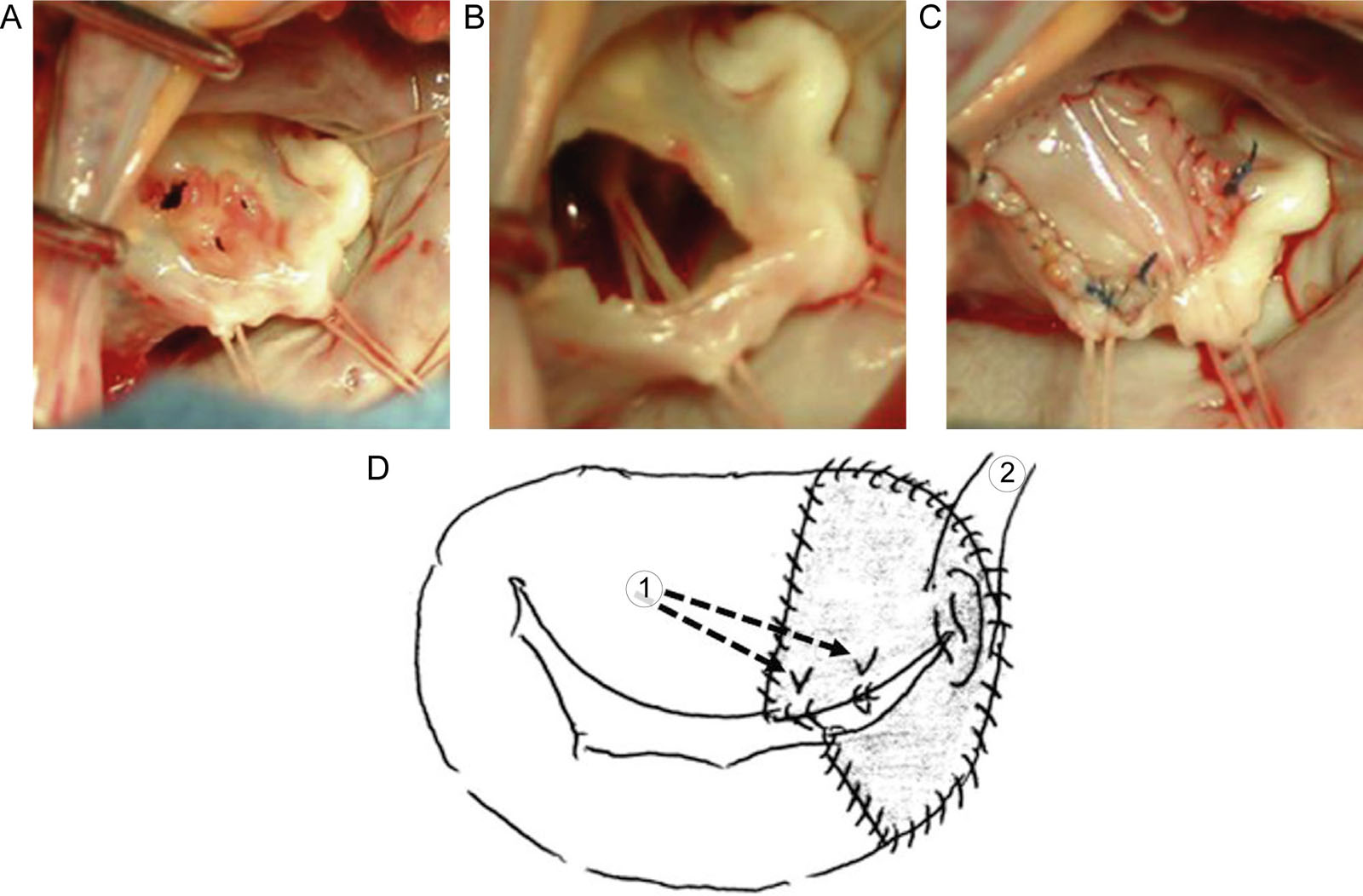
MV repair for infective endocarditis. These are intraoperative photos showing repair of the AMVL in a patient with endocarditis. (A) There are perforations of the AMVL requiring (B) resection of a portion of the AMVL. (C) Repair of the AMVL uses a patch closure of autologous pericardium. (D) Leaflet reconstruction using autologous pericardium and PTFE suture (*1: chordal reconstruction. *2: magic stitch to make a good coaptation). Abbreviations: AMVL, anterior mitral valve leaflet; MV, mitral valve; PTFE, polytetrafluorethylene. Adapted from Okada et al.30
eFigure 17.14
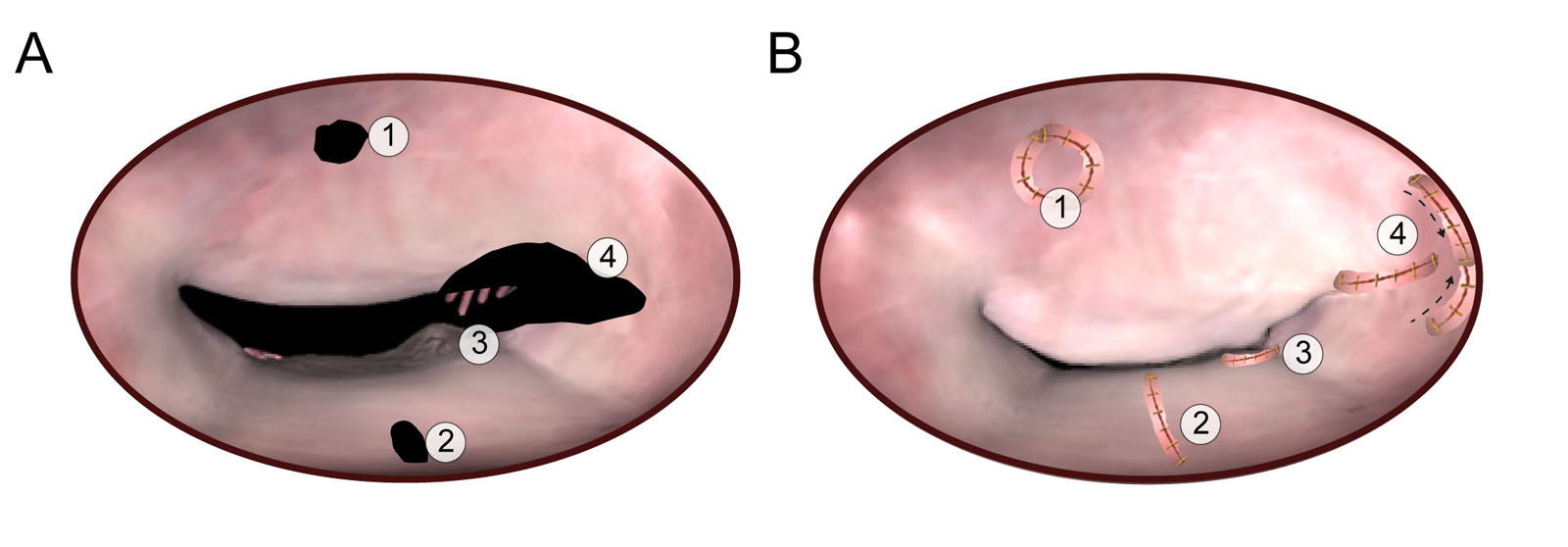
MV repair for infective endocarditis. These diagrams show different options for MV repair in endocarditis. (A) AMVL perforation treated by pericardial patch closure and PMVL quadrangular resection. (B) Pericardial patch replacement of almost the entire AMVL. (C) Chordal transposition from the PMVL to the free edge of the AMVL. (D) Sliding commissuroplasty for a prolapse of both AMVL and PMVL in the para-commissural area. Abbreviations: AMVL, anterior mitral valve leaflet; MV, mitral valve; PMVL, posterior mitral valve leaflet. Adapted from Dreyfus et al.31
eFigure 17.15
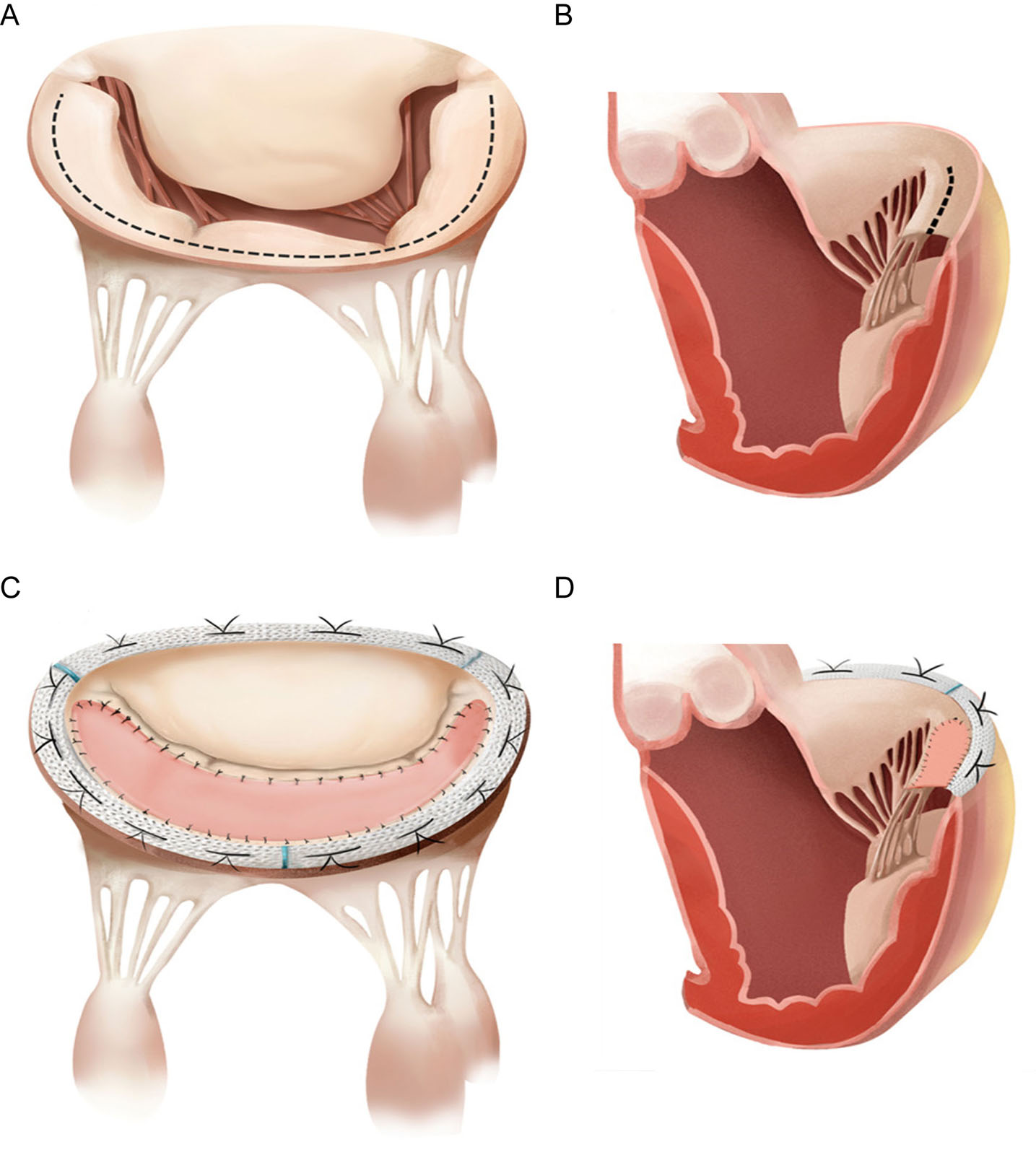
Secondary MR surgical approach. PMVL patch augmentation with true‐sized annuloplasty in patients with severe ischemic MR due to significant PMVL (i.e., P3) tethering. (A,B) A commissure‐to‐commissure incision is made along the posterior mitral annulus (the dashed line). (C,D) A CardioCel patch slightly larger than the space area succeeding the “fall” of the PMVL (whereas deferring to its shape and curvature) is prepared and sutured on the leaflet, followed by a true‐sized semirigid ring annuloplasty. Abbreviations: MR, mitral regurgitation; PMVL, posterior mitral valve leaflet. Adapted from Hu et al.102
eFigure 17.27
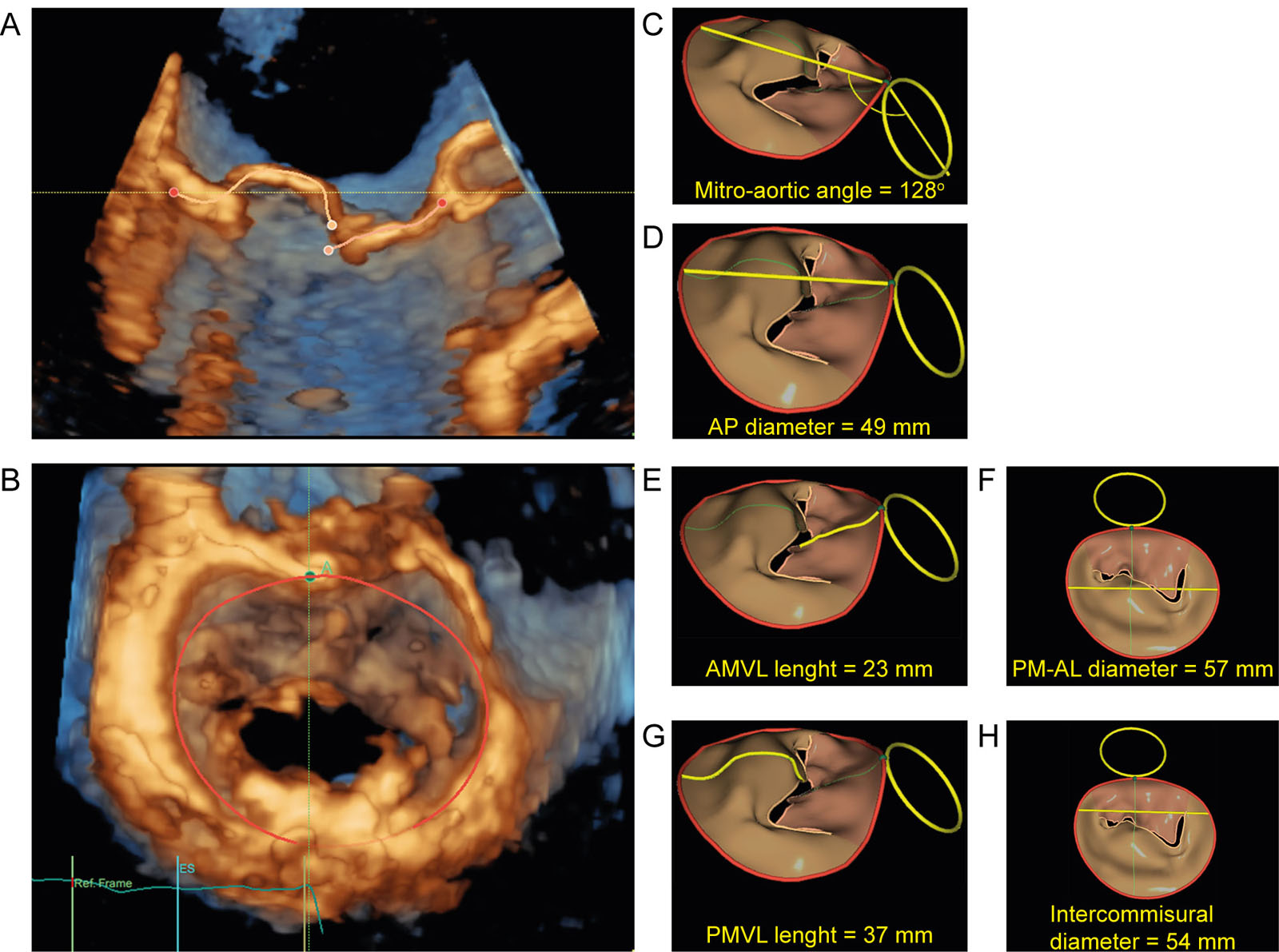
3D MV model measurements. (A, B) This is a 3D MV model obtained after computer analysis of 3D MV dataset which automatically gives measures of (C) mitro-aortic angle, (D) AP annulus diameter, (E )AMVL length, (F) PM-AL annulus diameter (G) PMVL length and (H) inter-commissural diameter. Abbreviations: 3D, three-dimensional; AL, antero-lateral; AMVL, anterior mitral valve leaflet; AP, antero posterior; MV, mitral valve; PM, postero-medial; PMVL, posterior mitral valve leaflet. (GE HealthCare, USA)
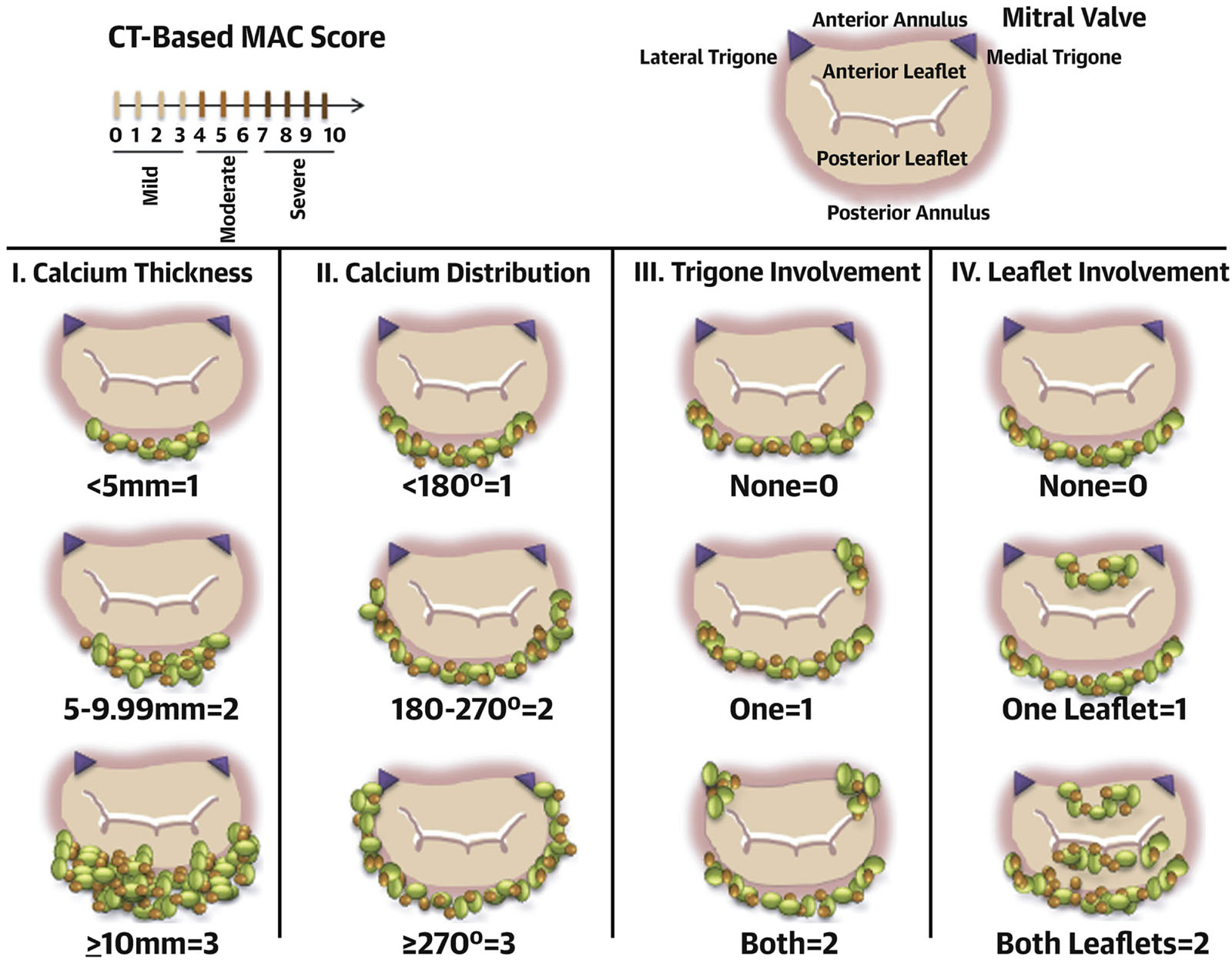
eFigure 17.28
MAC score. These diagrams illustrate the components of the MAC score and their corresponding points, including (I) average annulus calcium thickness, (II) calcium distribution in annulus circumference (III) trigone calcification and (IV) mitral leaflet calcification. A severity grade based on the total points accumulated as follows: mild MAC = 3 points or less, moderate MAC = 4 to 6 points, and severe MAC ≥ 7 points. Abbreviations CT, computed tomography; MAC, mitral annular calcification. Adapted from Guerrero et al.52
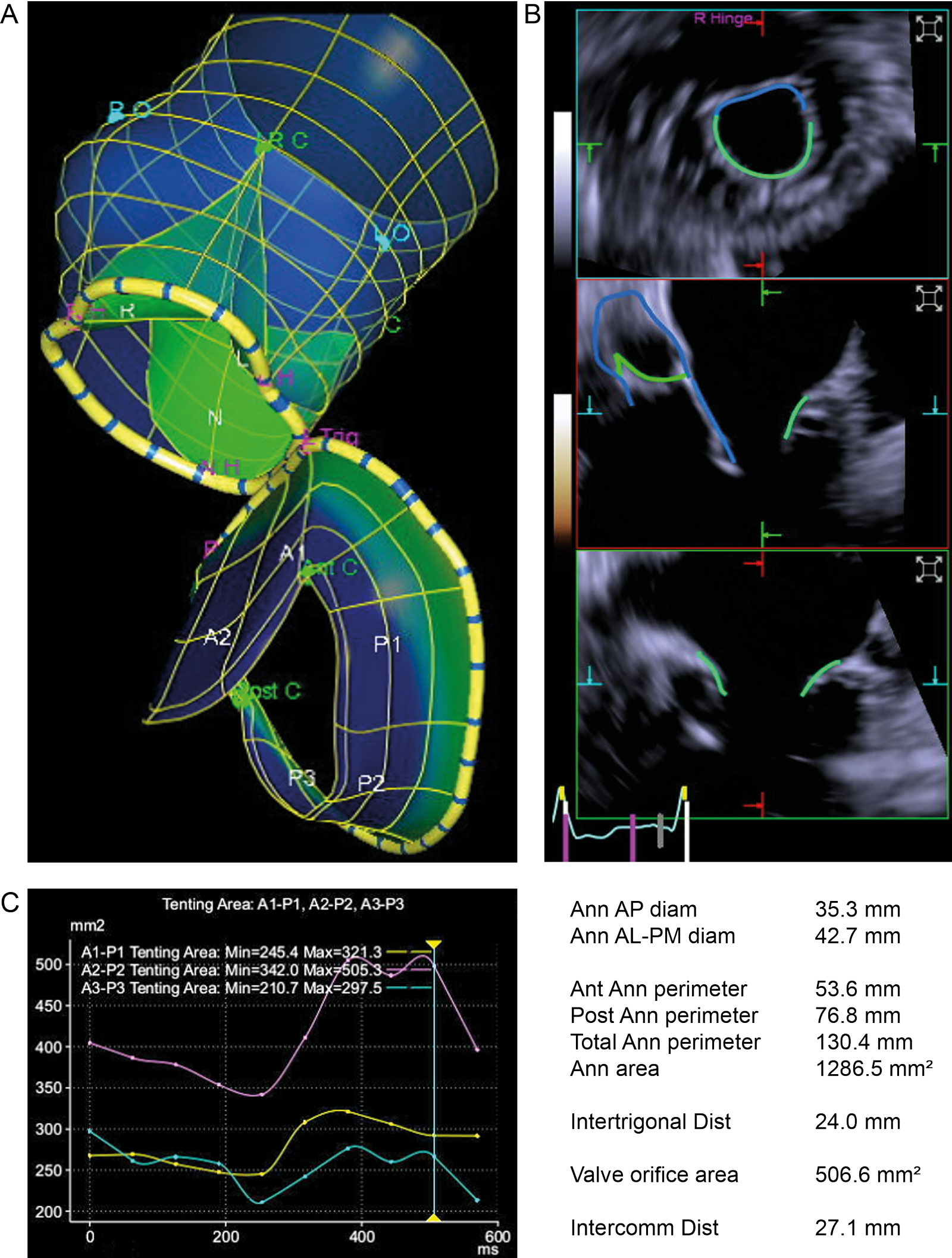
eFigure 17.34
AoV and MV 3D model. (A) This is an example of software analysis of a 3D dataset of the AoV and MV, which creates a single dynamic model. (B) The model automatically measures AoV and MV area, MV leaflet length and tenting area. (C) The measurements appear in graphic and numeric forms and can change during the cardiac cycle. Abbreviations: 3D, three-dimensional; AL, antero-lateral; Ann, annular; Ant, anterior; AoV, aortic valve; AP, anterior-posterior; Dist, distance; MV, mitral valve. (Siemens Healthinieers, Erlangen, Germany).
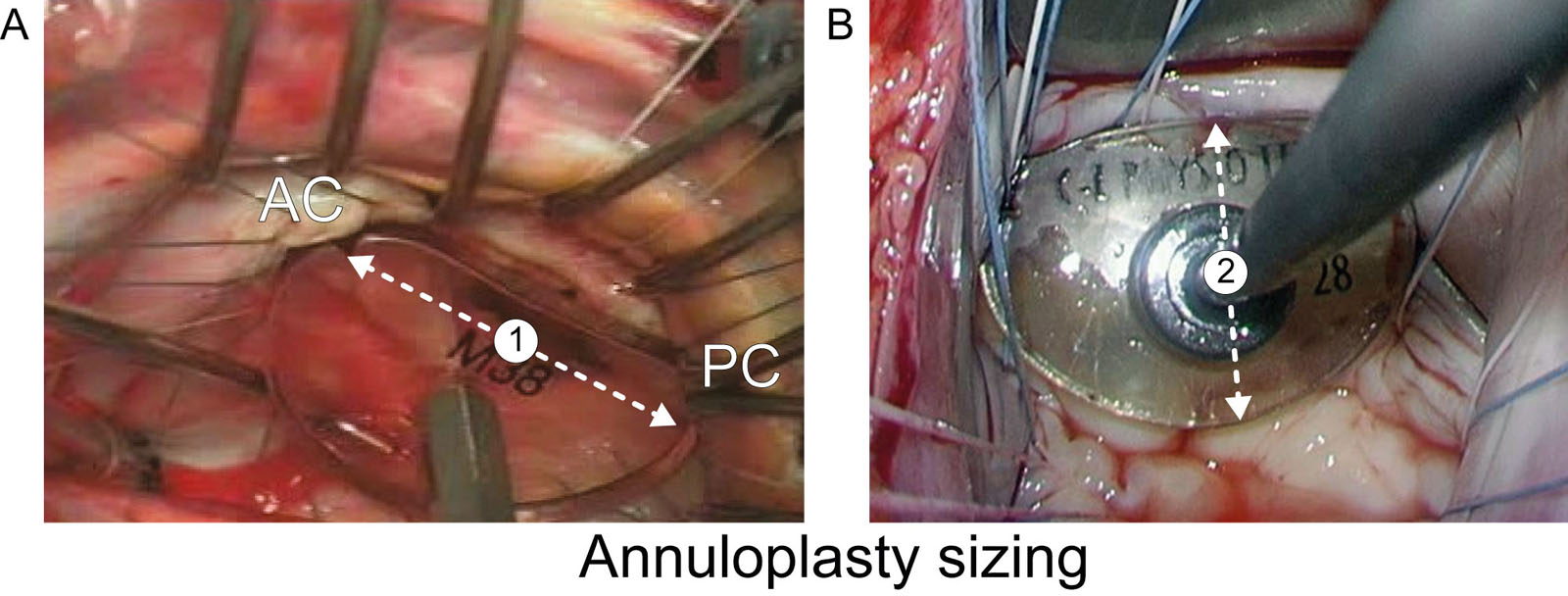
eFigure 17.35
Annuloplasty ring sizer. This illustration shows the different options for using the manufacturer’s sizer to determine the annuloplasty ring size. (A) Sizer notches for measuring either the inter-trigonal or inter-commissural distance (#1). (B) Area of the sizer to determine entire area of MV or bare area if anterior leaflet. The height measurement of the anterior leaflet (#2) is shown. Abbreviations: AC, anterior commissure; MV, mitral valve; PC, posterior commissure. Modified from Bothe et al. 62
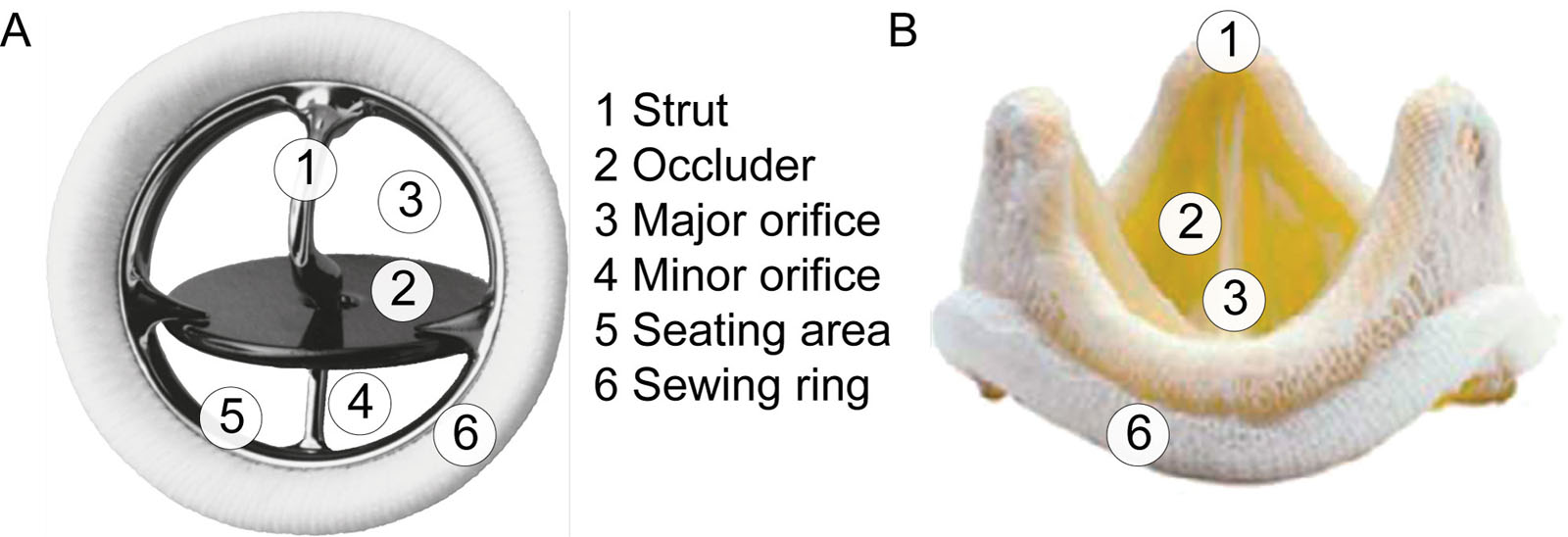
eFigure 17.41
Descriptors of the prosthetic valve components. (A) Mechanical tilting disc valve (Medtronic Hall, U.S.). (B) Bioprosthetic Epic™ Plus Mitral stented valve (Abbott, U.S.).
eFigure 17.49
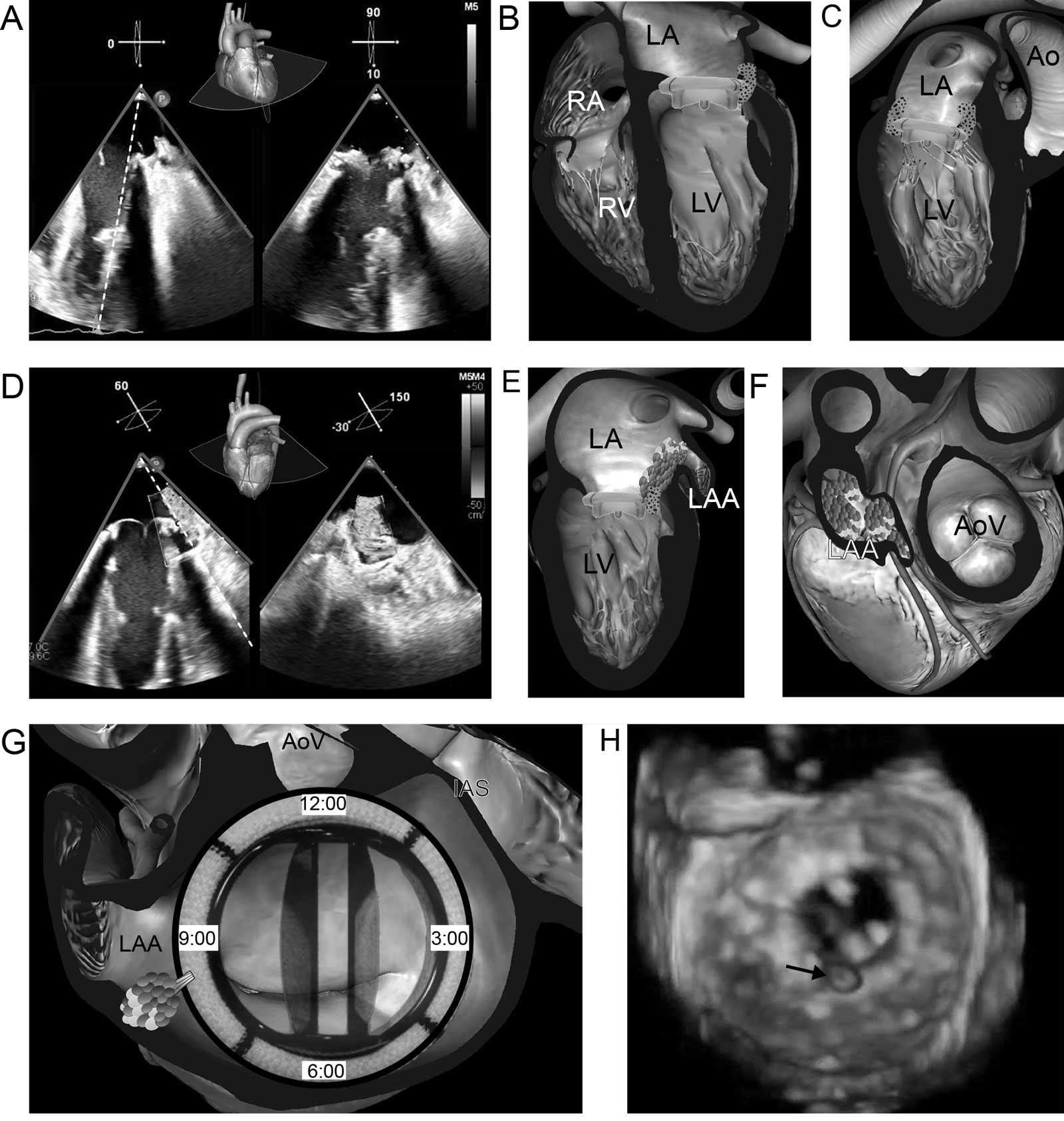
Bioprosthesis endocarditis. (A-C) Biplane ME 4C view shows abnormal leaflet irregular thickening (arrows) suggestive of vegetations. (D-F) Biplane ME 60° view with CFI shows valve dehiscence with regurgitation (arrows) extending into the LAA. (G) The location of the paravalvular leak is around 9 o’clock near the LAA ostium. (H) 3D view from the LA perspective of the prosthesis shows mobile vegetation (arrow). Abbreviations: 3D, three-dimensional; 4C, four-chamber; Ao, aorta; AoV, aortic valve; CFI, color flow imaging; LA, left atrium; LAA, left atrial appendage; LV, left ventricle; ME, mid-esophageal; RA, right atrium; RV, right ventricle.
eFigure 17.51
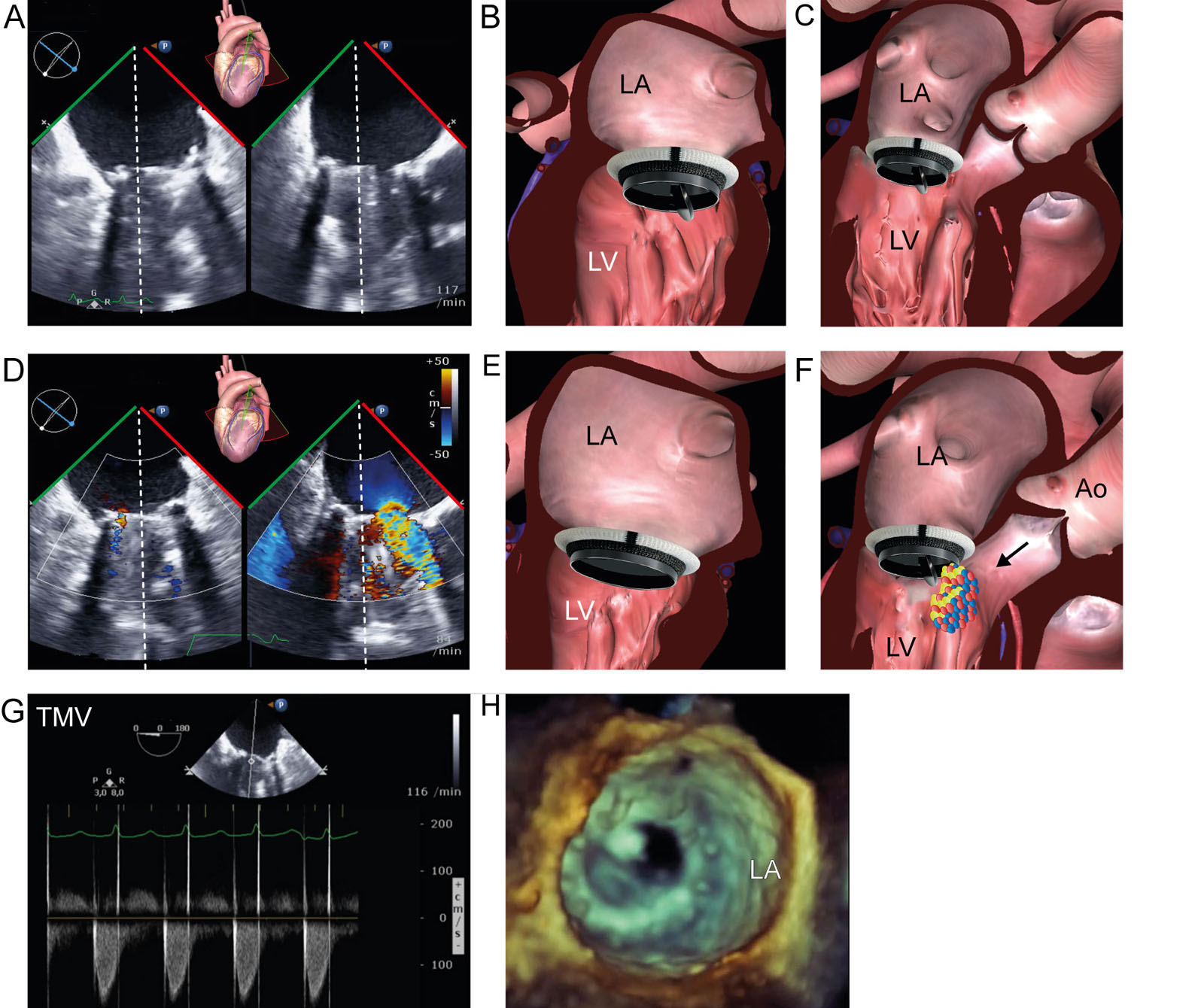
Prosthetic valve dysfunction. Bileaflet mechanical mitral valve prosthesis dysfunction. (A-C) Biplane ME MC view shows a bileaflet mechanical MV prosthesis during diastole with the posterior hemi-disc stuck in the closed position (arrows) 4 years after implantation. (D-F) Color compare ME MC view with CFI shows the stuck hemi-disc in the closed position with accelerated flow velocities across the other hemi-orifice. (G) CWD across the MV has an elevated diastolic gradient indicative of mitral stenosis. (H) 3D LA view of the mechanical MV prosthesis from the LA perspective confirms the stuck hemi-disc. Abbreviations: 3D, three-dimensional; Ao, aorta; CFI, color flow imaging; CWD, continuous wave Doppler; LA, left atrium; LV, left ventricle; MC, mid-commissural; ME, mid-esophageal; MV, mitral valve; TMV, transmitral velocity.
eFigure 17.52
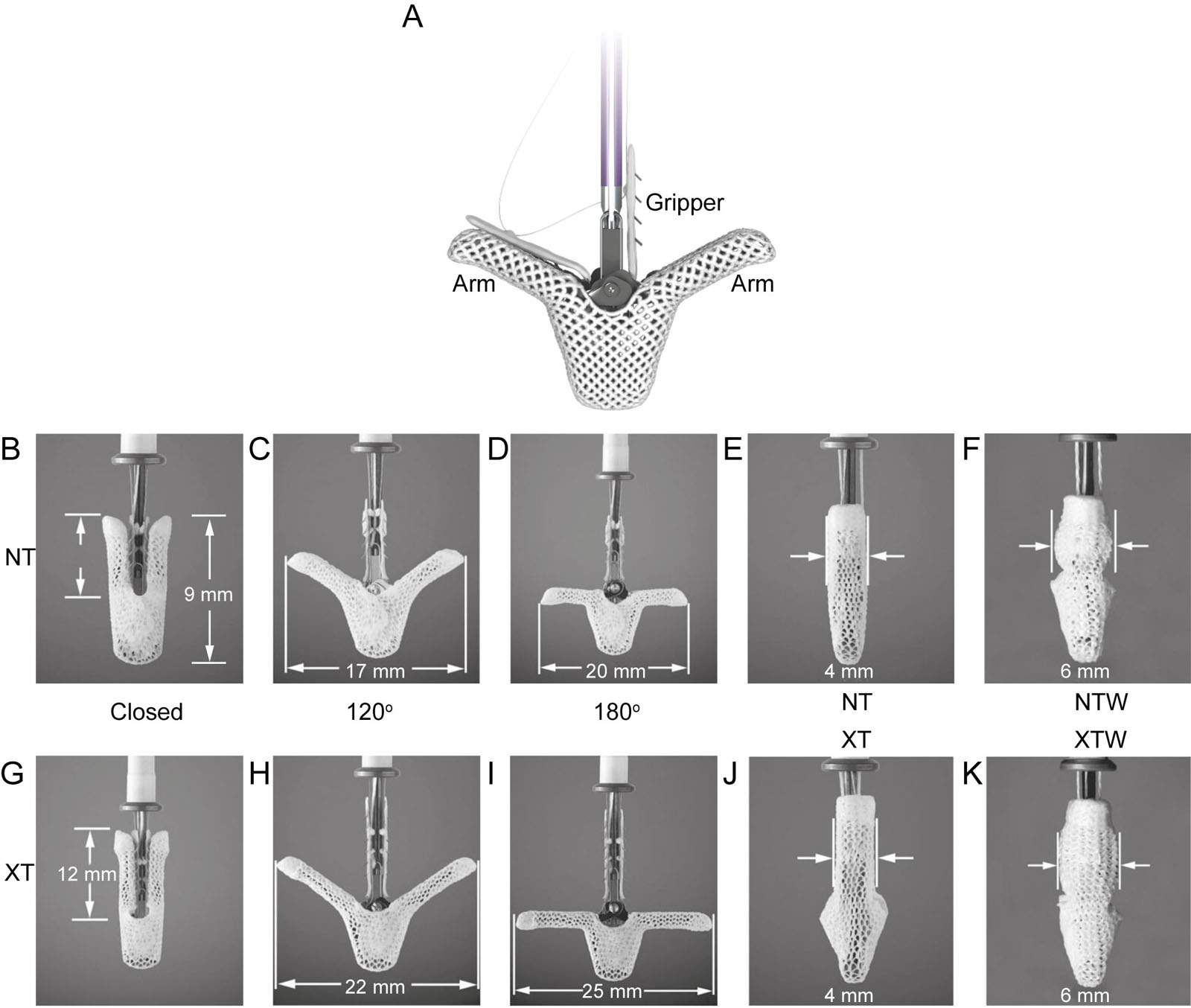
MitraClipTM devices. (A) This is a MitraClipTM used for transcatheter MV repair procedure to treat MR. These are photos of differentclips (A-F) NT and (G-K) XT which vary in size and clip opening angles. (Source: Abbott).
eFigure 17.53
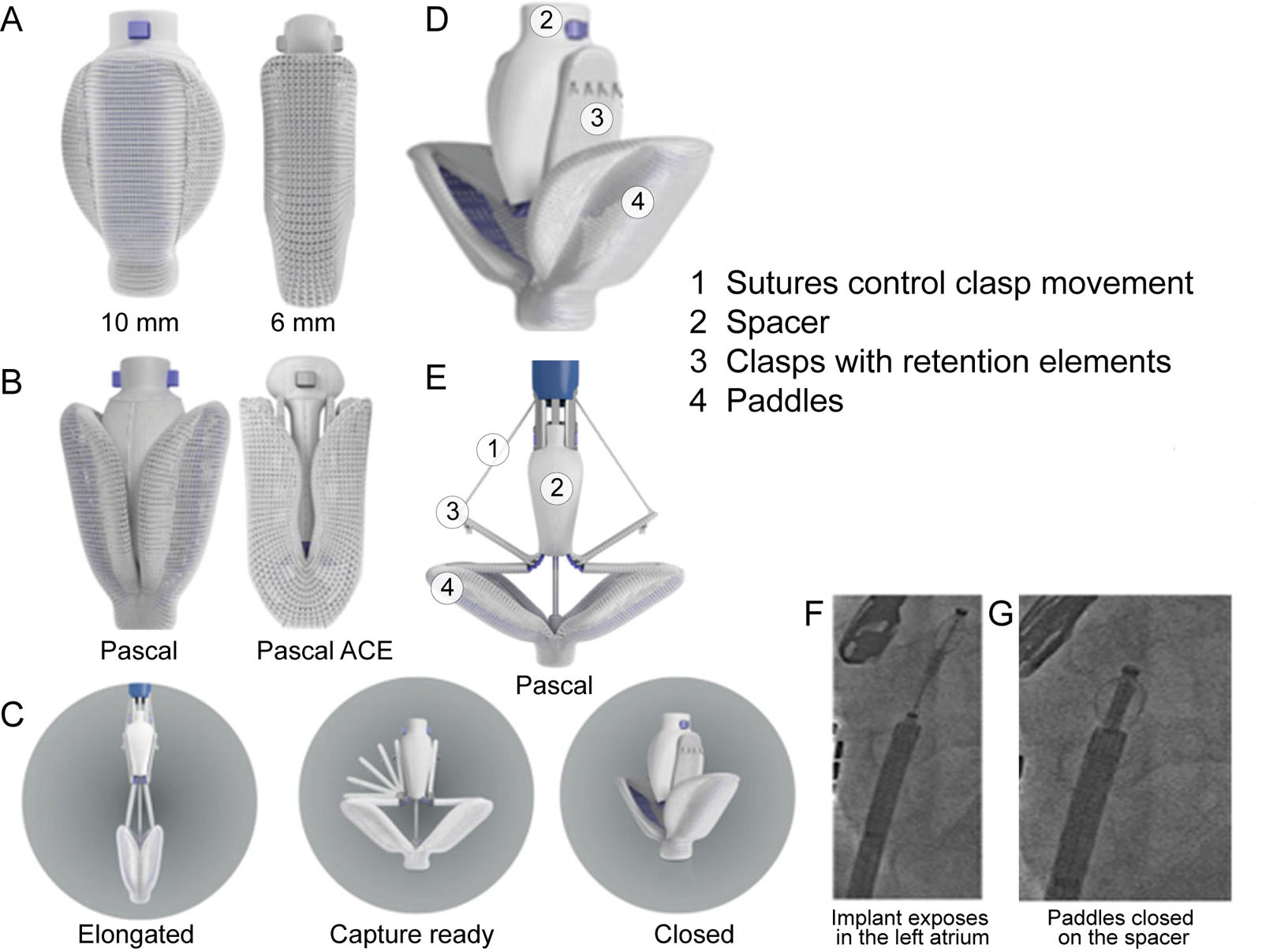
PASCAL® device. (A-G) These are photos of the different components and function of the Precision Transcatheter Valve Repair System (Edwards Lifesciences, Irvine, CA). Source modified from Whisenant et al. 104
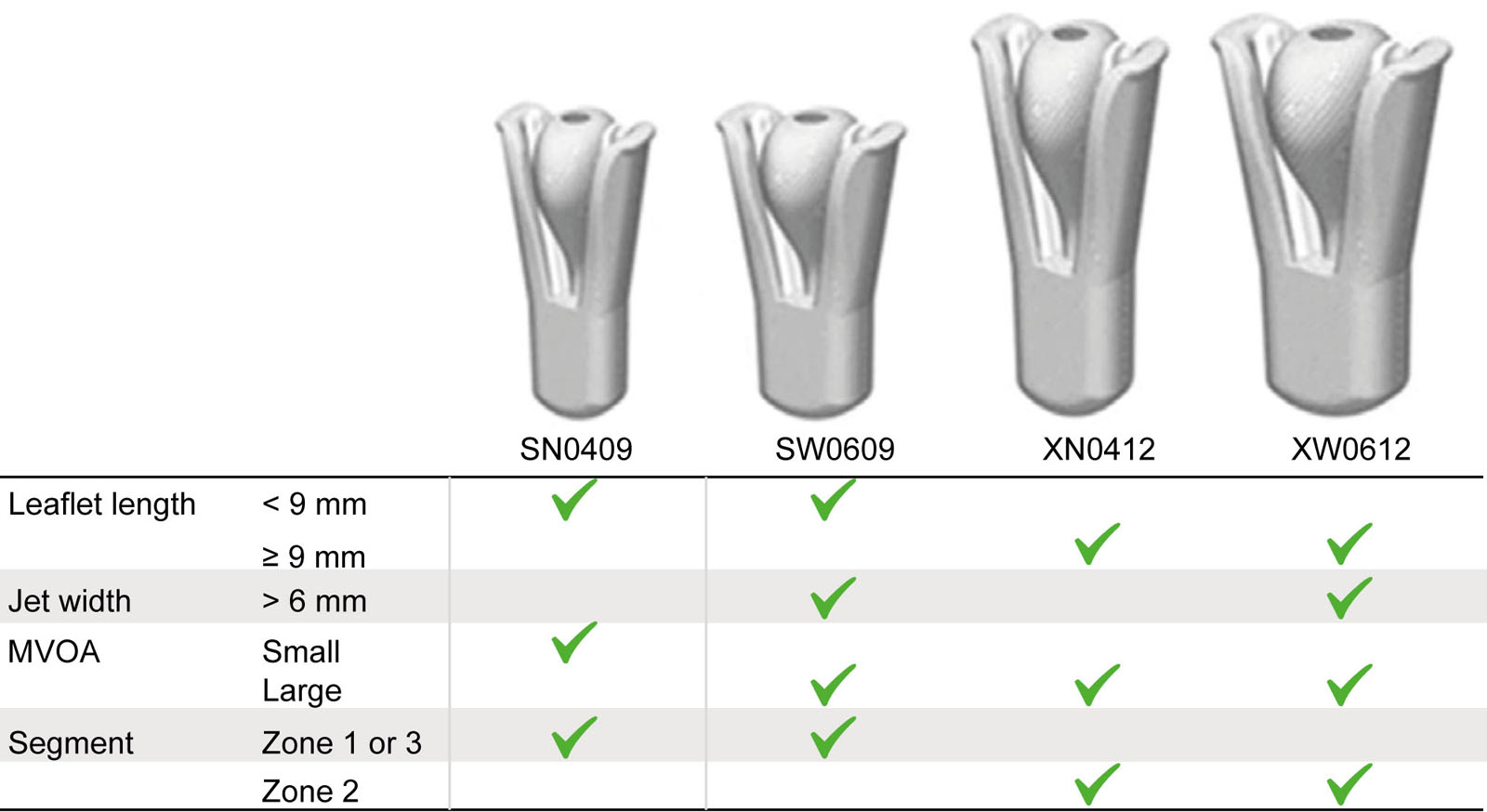
eFigure 17.55
DragonflyTM device. These illustrations show the DragonflyTM transcatheter MV repair device (Valgen Medtech, China) including the sizes and selection criteria. Abbreviations; MV, mitral valve; MVOA, mitral valve orifice area. Ref Liu X et al.105
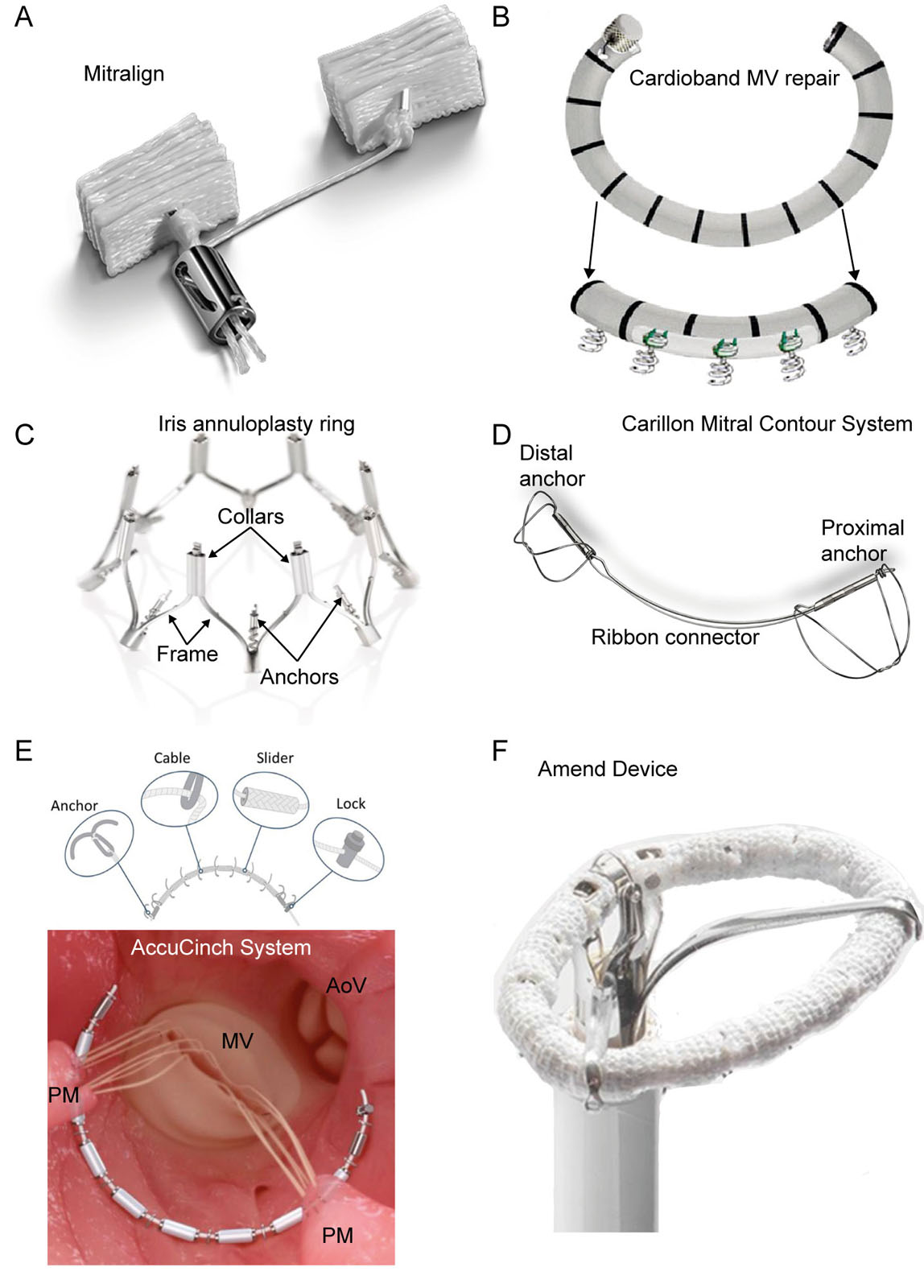
eFigure 17.64
Transcatheter MV repair systems. These are photos of percutaneous annuloplasty type devices for MV repair, including the (A) Mitralign System, (B) Cardioband Mitral Valve Repair System, (C) IRIS complete Annuloplasty Ring, (D) Carillon Mitral Contour System, (E) AccuCinch System, (F) Amend Device. Abbreviations: PM, papillary muscle; MV, mitral valve; AoV, aortic valve.
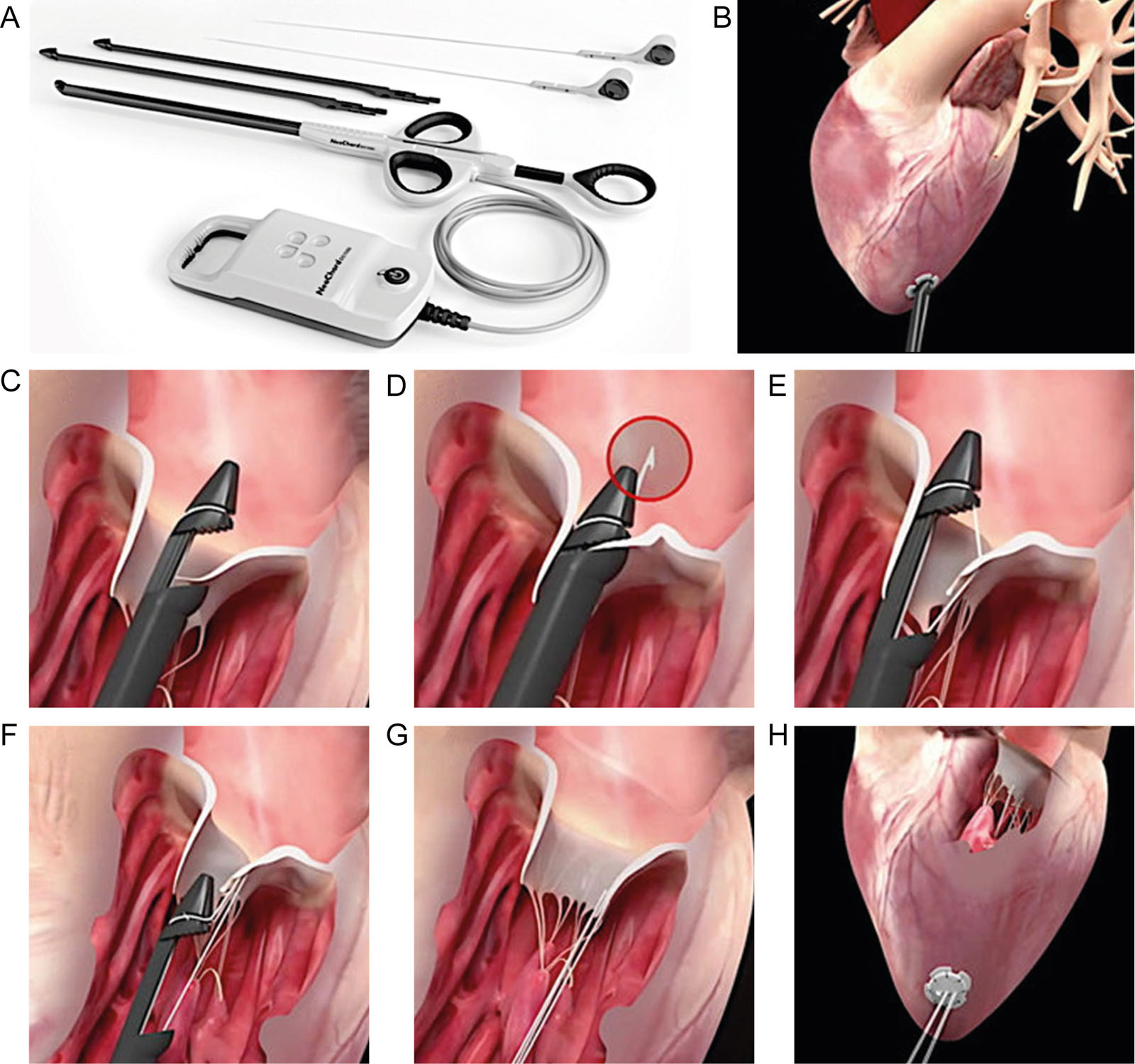
eFigure 17.65
Transcatheter MV repair system. This figure describes the (A) Neochord system for transcatheter mitral valve repair with insertion (B) through the LV apex. (C) Once the tip has crossed the valve, the jaws are opened, and the leaflet edge is grasped by withdrawing the device from the LA. (D, E) The leaflet is pierced through a needle and a loop of the suture is deployed. (F, G) The device is retrieved, exteriorizing the chordal loop; a girth hitch knot is formed. (H) The length of each neo‐chordae is set until adequate coaptation is reached, under real‐time TEE; each of the neo‐chordae is fixed to an epicardial Teflon pledget. Abbreviations: LA, left atrium; LV, left ventricle; MV, mitral valve; TEE, transesophageal echocardiography. With permission from D’Onofrio et al. 85 With permission of neochord DS1000 System (Neochord, Inc).
eFigure 17.67
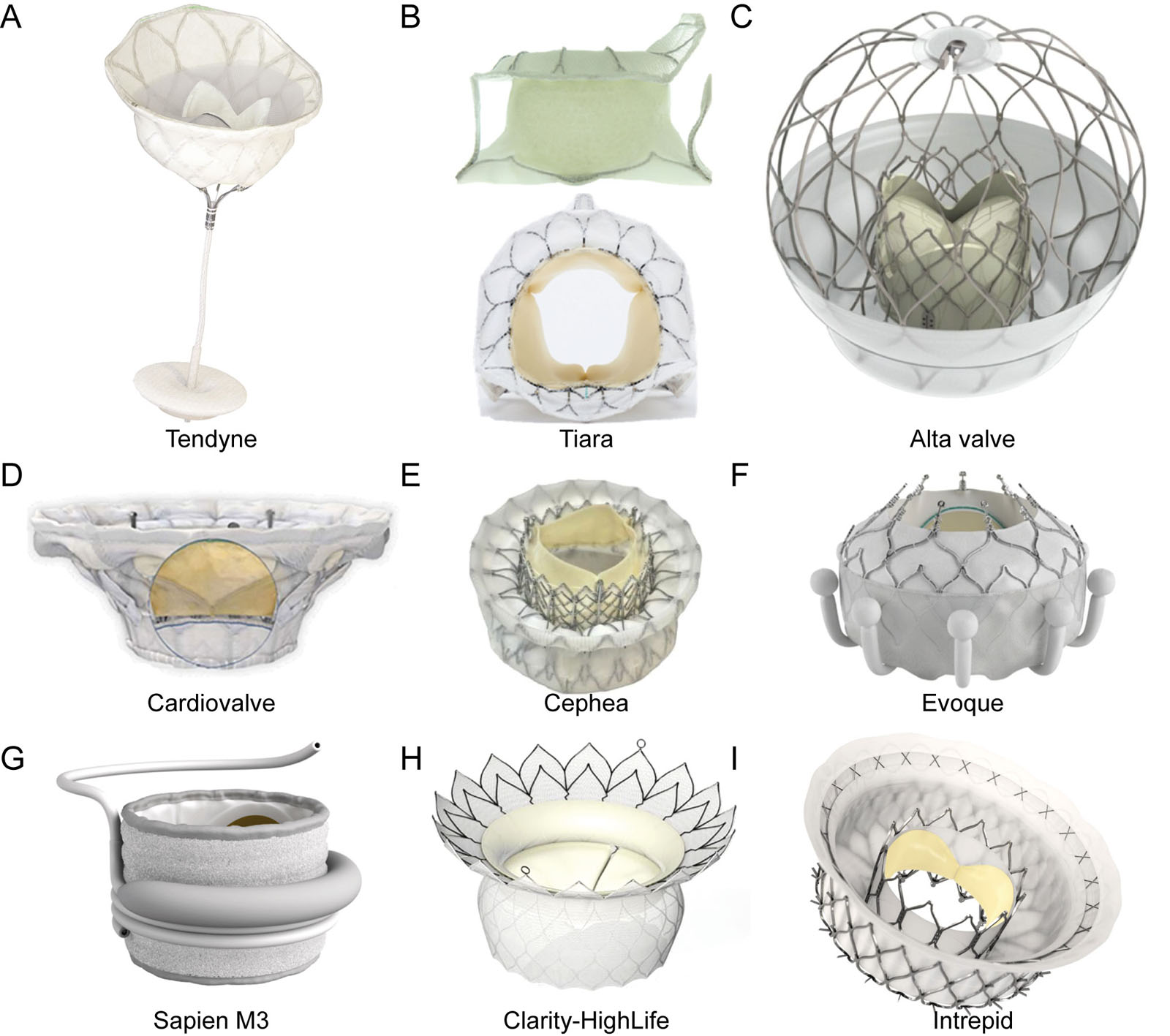
eFigure 17.67 Transcatheter MV bioprosthesis. These are photos of the different percutaneous transcatheter MV bioprostheses including .
Transapical Systems. A-Tendyne® (Abbott Vascular, Santa Clara, CA, USA) is a fully repositionable and retrievable TMVR device with two Nitinol stents housing a trileaflet porcine pericardial valve with an adjustable tether, apical fixation and sealing pad. The inner stent is circular, while the outer stent is D-shaped to replicate the native annulus. Valve insertion uses a transapical approach, with partial deployment in the LA and progressive withdrawal to the annulus before complete deployment. A tether tensioned to an apical pad sets the valve in position. Successful implantation occurred in 96% of the first 100 patients. Thirty-day mortality was 26%, disabling stroke 3%, and reintervention 3%. There was 99% complete MR resolution at 30 days, 98% at one year and 93% at two years with a trans-prosthetic diastolic mean gradient of 3.2 mmHg. The SUMMIT trial (NCT03433274) is ongoing (eFigure 17.67A).
B-Tiara®. (NeoVasc, Richmond, British Columbia, Canada) entails a trileaflet bovine pericardial valve mounted in a self-expanding Nitinol alloy with an asymmetrical D-shaped design. Delivery uses a transapical approach but with a different ventricular anchoring system compared to the Tendyne® valve. Successful implant occurred in 92% of patients across the TIARA-I and TIARA-II studies. Thirty-day mortality was 12.3%, and 88% of patients had no or trace MR at discharge (eFigure 17.67B).
Transseptal Systems.
C-AltaValve (4C Medical Technologies, Maple Grove, MN, USA) is a unique valve placed in a supra-annular LA position rather than the mitral annulus. This atrial-only fixation design lessens the risk of device embolization, LVOT obstruction and LV dysfunction from chordal rupture. It features a self-expanding spherical nitinol frame sized to fit the LA, housing a 27-mm bovine pericardial valve with a fabric skirt at the annular ring level to enhance tissue growth and minimize peri-prosthetic regurgitation. There are reports of first-in-human cases106 and an early feasibility study (NCT03997305) is under way. Current limitations include LA dimensions > 90 mm at baseline and an MV annular dimension < 29 mm. (eFigure 17.67C).
D-Cardiovalve. (Valtech / Or Yehuda, Israel) is a self-expanding bovine pericardial trileaflet valve with atrial and ventricular frames. Early data showed 100% successful implantation, with 80% of patients having no post-procedural MR. Thirty-day mortality was 60%, primarily from access-site complications (eFigure 17.67D).
E-Cephea (Abbott Vascular) has a self-expanding double-atrial and ventricular disk design, with an inner ring holding a trileaflet bovine pericardial valve. First-in-human experience showed successful implantation without complications but await further clinical data (eFigure 17.67E).
F-Evoque. (Edwards Lifesciences, Irvine, CA, USA) is a self-expanding nitinol valve with bovine pericardial leaflets. Its ventricular frame incorporates nine anchors, and the atrial frame includes a sealing skirt. Early data in 14 patients showed technical success in 93%, with mild or no MR in 83% of patients (eFigure 17.67F).
G-SAPIEN M3 (Edwards Lifesciences, Irvine, CA, USA) comprises a nitinol dock encircling the MV apparatus, placed within a 29-mm balloon-expandable valve. Early compassionate use in 35 high-risk patients showed technical success in 89%. Thirty-day mortality was 3%, with mild or less MR in 88% of patients (Figure e17.67G).
H-HighLife (HighLife Medical, Paris, France) uses a valve-in-ring concept with a subannular ring anchoring the self-expanding trileaflet bovine pericardial valve. The MV subvalvular apparatus is first encircled under fluoroscopic and TEE guidance by a guidewire introduced retrograde from peripheral arterial access. After confirming the appropriate position, there is implantation of a subannular ring over the guidewire. a transseptal approach delivers the bioprosthesis with the ring acting as a ventricular anchor. Early feasibility study data (HL-2018-01) showed successful implantation in 46 of 52 patients (88%). Thirty-day all-cause mortality was 13.5 % (Figure e17.67H).
I-Intrepid (Medtronic, Minneapolis, MN, USA) system features a dual-stent, symmetric design. The conformable outer stent engages the annulus and leaflets, providing fixation and sealing, while the inner stent houses a 27-mm tricuspid bovine pericardial valve. A large flexible brim aids imaging during implantation and subsequent tissue in-growth. Despite using a transseptal approach, valve deployment is first from the atrial side followed by complete unsheathing of the ventricular side. This system originally used a transapical approach. The APOLLO trial (NCT03242642) with transseptal delivery is underway, up to 1350 patients enrolled, including a cohort of 300 patients with MAC (eFigure 17.67I). Abbreviations: LA, left atrial; LV, left ventricle; LVOT, left ventricular outflow tract; MR, mitral regurgitation; MV, mitral valve; TEE, transesophageal echocardiography; TMVR, transcatheter mitral valve replacement.
Videos
Chapter 17 Fig01A
Chapter 17 Fig01C
Chapter 17 Fig02A
Chapter 17 Fig03A
Chapter 17 Fig03C
Chapter 17 Fig07BDFH
Chapter 17 Fig10B
Chapter 17 Fig11A
Chapter 17 Fig19E
Chapter 17 Fig20AEH
Chapter 17 Fig20AEI
Chapter 17 Fig20B
Chapter 17 Fig20B1
Chapter 17 Fig20B2
Chapter 17 Fig20CFI
Chapter 17 Fig20DGJ
Chapter 17 Fig20DHL
Chapter 17 Fig21A
Chapter 17 Fig21B
Chapter 17 Fig21C
Chapter 17 Fig21D
Chapter 17 Fig22A
Chapter 17 Fig22B
Chapter 17 Fig22D
Chapter 17 Fig23A
Chapter 17 Fig23B
Chapter 17 Fig25BDF
Chapter 17 Fig29A
Chapter 17 Fig29E
Chapter 17 Fig32
Chapter 17 Fig34A
Chapter 17 Fig36A
Chapter 17 Fig36B
Chapter 17 Fig38A
Chapter 17 Fig38D
Chapter 17 Fig39A
Chapter 17 Fig39B
Chapter 17 Fig40A
Chapter 17 Fig40B
Chapter 17 Fig40E
Chapter 17 Fig40F
Chapter 17 Fig42AB
Chapter 17 Fig42CD
Chapter 17 Fig42EF
Chapter 17 Fig43A
Chapter 17 Fig43B
Chapter 17 Fig44A
Chapter 17 Fig44E
Chapter 17 Fig45A
Chapter 17 Fig45B
Chapter 17 Fig46A
Chapter 17 Fig46C
Chapter 17 Fig46H
Chapter 17 Fig47B
Chapter 17 Fig47C
Chapter 17 Fig49H
Chapter 17 Fig50A
Chapter 17 Fig50D
Chapter 17 Fig50H
Chapter 17 Fig51A
Chapter 17 Fig51D
Chapter 17 Fig51H
Chapter 17 Fig53
Chapter 17 Fig54ADEH
Chapter 17 Fig57A
Chapter 17 Fig57C
Chapter 17 Fig57D
Chapter 17 Fig58A
Chapter 17 Fig58D
Chapter 17 Fig59A
Chapter 17 fig59D
Chapter 17 Fig60A
Chapter 17 Fig60C
Chapter 17 Fig60D
Chapter 17 Fig60E
Chapter 17 Fig61A
Chapter 17 Fig61B
Chapter 17 Fig62A
Chapter 17 Fig62B
Chapter 17 Fig63A
Chapter 17 Fig63D
Chapter 17 Fig66AC
Chapter 17 Fig66B
Chapter 17 Fig66D
Chapter 17 Fig67A
Chapter 17 Fig67C
Chapter 17 Fig67D
Chapter 17 Fig67H
Tables
eTable 17.1 Scores in assessing MV anatomy
| Wilkins Scorea 3 | |||||
| Grade | Leaflet mobility | Valve thickness | Calcification | Subvalvular thickening | |
| 0 | Normal | Normal leaflet thickness | None | None | |
| 1 | Highly mobile valve with only leaflets tips restricted | Leaflets near normal in thickness (4–5 mm) | A single area of increased echo brightness | Minimal thickening just below mitral leaflets | |
| 2 | Leaflet mid and base portions have normal mobility | Mid-leaflets normal, considerable thickening of margins (5–8 mm) | Scattered areas of brightness confined to leaflet margins | thickening of chordal structures extending up to one third of chordal length | |
| 3 | Valve continues to move forward in diastole, mainly from the base | Thickening extending through entire leaflet (5–8 mm) | brightness extending into mid-portion of leaflets | Thickening extending to distal third of chords | |
| 4 | No or minimal forward movement to leaflets in diastole | Considerable thickening of all leaflet tissue (>8–10 mm) | Extensive brightness throughout much of leaflet tissue | Extensive thickening and shortening of all chordal structures extending down to papillary muscles | |
| Cormier score 93 | |||||
| Echocardiographic group | MV anatomy | ||||
| Group 1 | Pliable noncalcified MVAL and mild subvalvular disease (i.e., thin chordae ≥10 mm long) | ||||
| Group 2 | Pliable noncalcified MVAL and severe subvalvular disease (i.e., thickened chordae <10 mm long) | ||||
| Group 3 | MV calcification of any extent, assessed by fluoroscopy, whatever the state of subvalvular apparatus | ||||
| Echo score revisited for immediate outcome prediction b 5 | |||||
| Echocardiographic variable | Points for score (0 to 1) | ||||
| MV area ≤ 1 cm² | 2 | ||||
| Maximal leaflet displacement ≤ 12 mm | 3 | ||||
| Commissural area ratio ≥ 1.25 | 3 | ||||
| Subvalvular involvement | 3 | ||||
| aEach of the four characteristics is given a score from 0 to 4, with results ranging from 0 to 16. b Risk groups: low (score 0-3); intermediate (score 4-5); high (score 6-11) Abbreviations: MV, mitral valve; MVAL, mitral valve anterior leaflet. Adapted from Baumgartner et al. 2 | |||||
eTable 17.5 Unfavorable characteristics for MV repair in secondary MR on TTE
| Mitral valve deformation Coaptation distance (leaflet tenting height) ≥ 1 cm Leaflet tenting area >2.5–3 cm2 Complex jets originating centrally and postero-medially Postero-lateral angle >450 (severe posterior leaflet tethering)a Local LV remodeling Interpapillary muscle distance >20 mm Posterior papillary-fibrosa distance >40 mm Lateral wall motion abnormality Global LV remodeling LVEDD >65 mm, LVESD >51 mm (LVESV >140 mL) (low likelihood of reverse LV remodeling after repair and poor long-term outcome) Systolic sphericity index >0.7 |
| a Measure the tethering angle at P3 using MPR analysis of a 3D MV dataset (Figure 17.30). Tethering angle > 30° at the P3 level of TEE is unfavorable for MV repair.96 |
| Abbreviations: 3D, three-dimensional; LV, left ventricle; LVEDD, left ventricular end-diastolic diameter; LVESD, left ventricular end-systolic diameter; LVESV, left ventricular end-systolic volume; MPR, multiplane reconstruction; MR, mitral regurgitation; MV, mitral valve; TEE, transesophageal echocardiography; TTE, transthoracic echocardiography. From Lancelotti et al. 95 |
eTable 17.8 Normal reference values of EOA for prosthetic MV
| Prosthetic MV | 25 | 27 | 29 | 31 | 33 |
| Stented bioprosthesis valves (cm2) | |||||
| Medtronic mosaic | 1.5±0.4 | 1.7±0.5 | 1.9±0.5 | 1.9±0.5 | |
| Hancock II | 1.5±0.4 | 1.8±0.5 | 1.9±0.5 | 2.6±0.5 | 2.6±0.7 |
| CE Perimount | 1.6±0.4 | 1.8±0.4 | 2.1±0.5 | ||
| Mechanical valves (cm2) | |||||
| St-Jude MS | 1.5±0.3 | 1.7±0.4 | 1.8±0.4 | 2.0±0.5 | 2.0±0.5 |
| MCRI On-Xa | 2.2±0.9 | 2.2±0.9 | 2.2±0.9 | 2.2±0.9 | 2.2±0.9 |
| aThe On-X valve has just 1 size for 27 to 29 and 31 to 33 mm prostheses. In addition, the strut and leaflets are identical for all sizes (25 to 33 mm); only the size of the sewing cuff is. | |||||
| Abbreviations: CE, Carpentier-Edwards; EOA, effective orifice area; MS Medical Standard; MV, mitral valve. Adapted from Pibarot97 and Lancelotti et al.76 | |||||
eTable 17.10. Favorable and unfavorable criteria for TEER
| Criteria | Ideal Simple | Suitable Complex | Challenging Very complex | Hard or impossible | |
| Location | A2 / P2 | A1 / P1 or A3/P3 | Commissural lesion with multiple jets Wide jet involving the whole coaptation | Multiple segments Deep regurgitant cleft or leaflet perforation | |
| Calcification | None | Annular calcification without leaflet involvement | Annular calcification with leaflet involvement | Concentric MAC with stenosis | |
| Grasping zone obstacle | Calcification in grasping zone | ||||
| Maximal MVA (MPR planimetry) | > 4 cm2 | 3.5-4.0 cm2 | 3.0-3.5 cm2 | < 3 cm2 | |
| Diastolic MG | > 5 mmHg | ||||
| PMVL Length | > 10 mm | 7 – 10 mm | 5 – 7 mm | < 5 mm | |
| Leaflet mobility & thickness | Normal | Asymmetric tethering | Barlow’s disease, Fibrotic leaflets, Cleft | Rheumatic thickening | |
| Tenting height (FMR) | < 10 mm | > 10 mm | > 10 mm | > 10 mm | |
| Flail width (DMR) Flail gap (DMR) | < 15 mm < 10 mm | > 15 mm > 10 mm | > 15 mm > 10 mm | > 15 mm > 10 mm | |
| Other | 2 jets from leaflet indentations Coaptation reserve <3 mm98 Leaflet-to-annulus index <1.2 99 | Failed surgical annuloplasty | |||
| * Favors replacement. Abbreviations: DMR, degenerative mitral regurgitation; FMR, functional mitral regurgitation; MAC, mitral annular calcification MPR, multiplane reconstruction; MVA, mitral valve area; Adapted from Hausleiter et al100 | |||||