Figures
eFigure 18.9
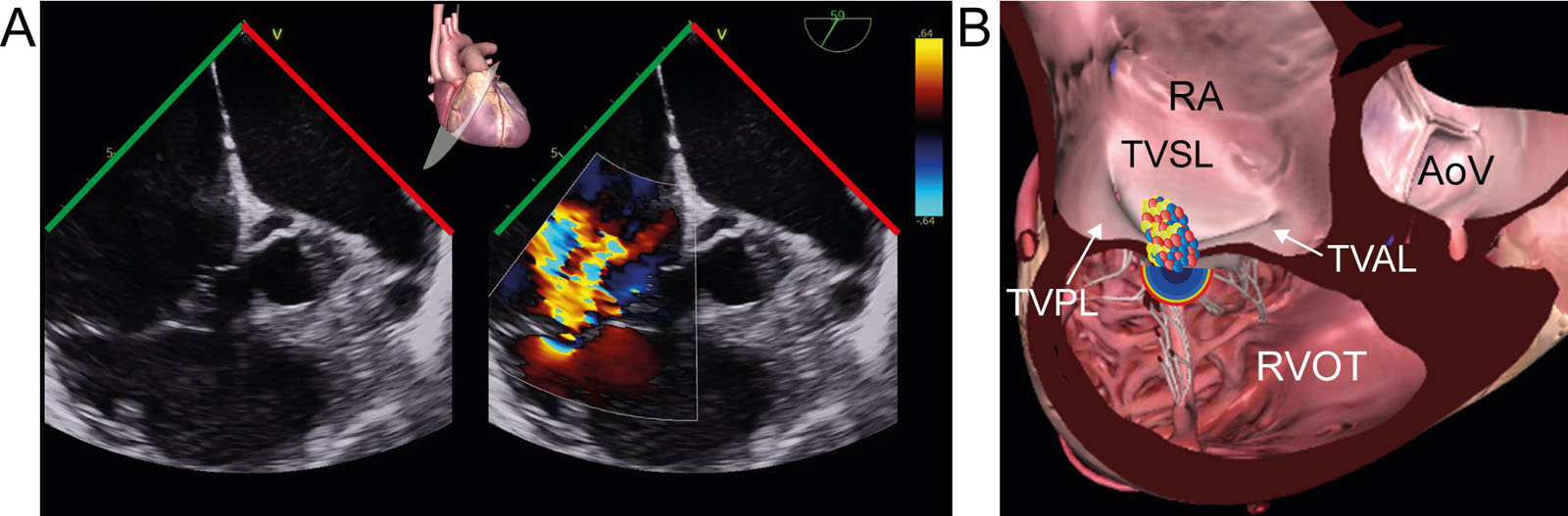
DE right ventricular inflow/outflow view of the TV. (A,B) This color compare DE view shows both the TVPL and TVAL with and without CFI. (C) This is a diagram of the TV from the RA perspective in the surgeon’s orientation, showing the plane. Abbreviations: AoV, aortic valve; CFI, color flow imaging; DE, deep esophageal; RA, right atrium; RVOT, right ventricular outflow tract; TV, tricuspid valve; TVAL, tricuspid valve anterior leaflet; TVPL, tricuspid valve posterior leaflet; TVSL, tricuspid valve septal leaflet.
eFigure 18.12
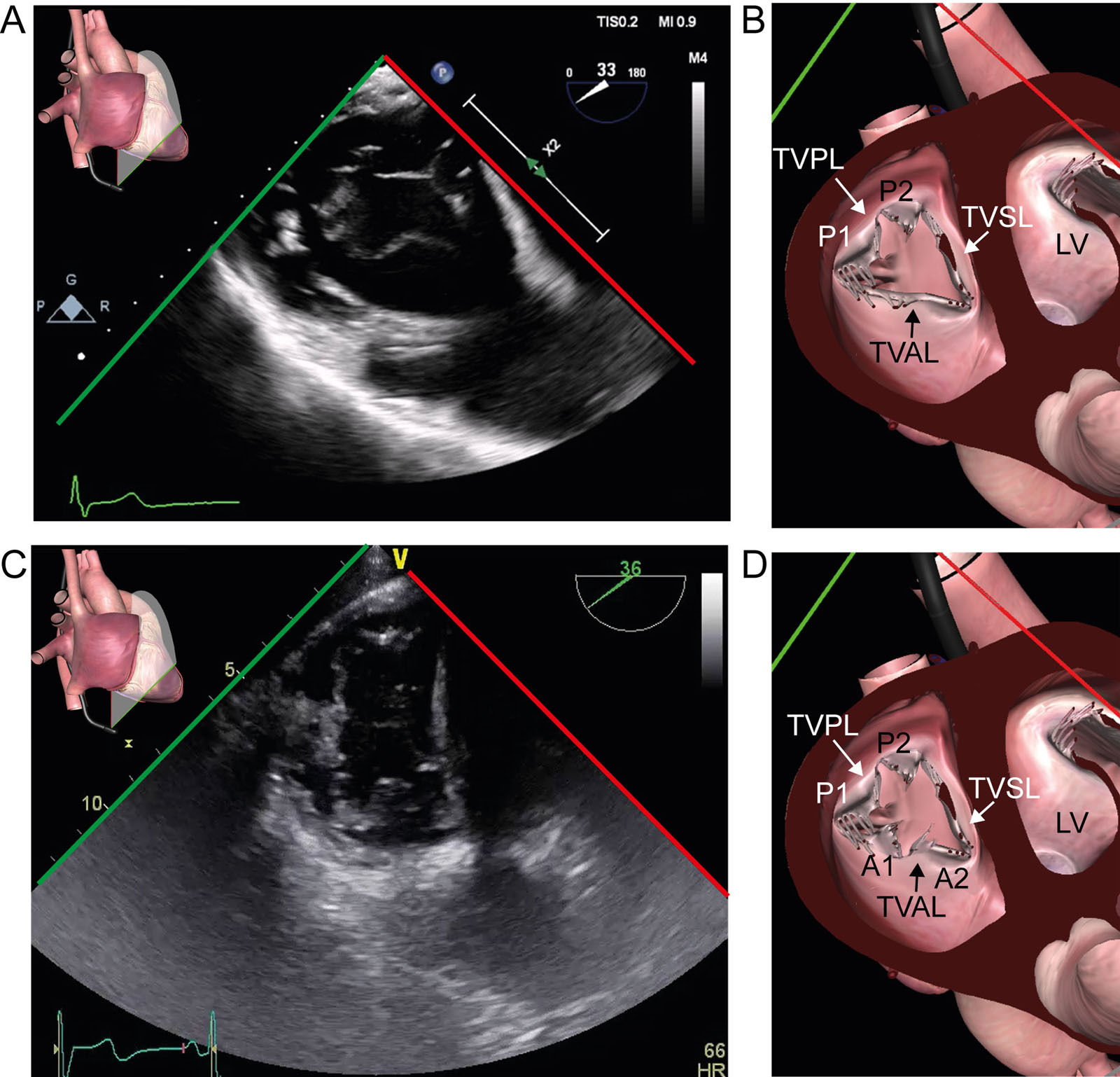
TV anatomic variants. (A-D) These TG basal views of the TV show (A, B) type IIIB with two posterior leaflets and (C, D) type IV with 2 anterior and 2 posterior leaflets. Abbreviations: A, anterior; LV, left ventricle; P, posterior; TG, transgastric; TV, tricuspid valve; TVAL, tricuspid valve anterior leaflet; TVPL, tricuspid valve posterior leaflet; TVSL, tricuspid valve septal leaflet.
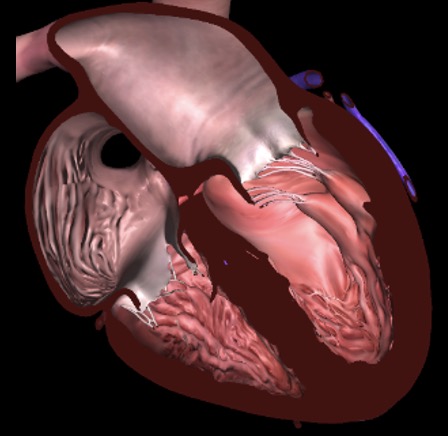
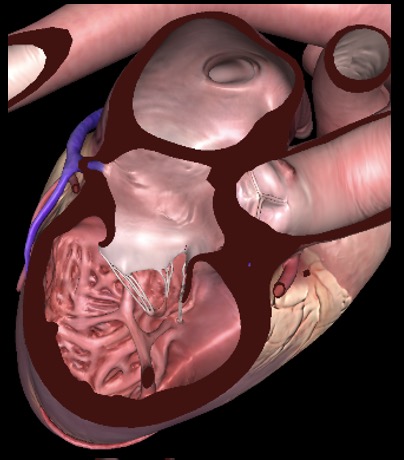
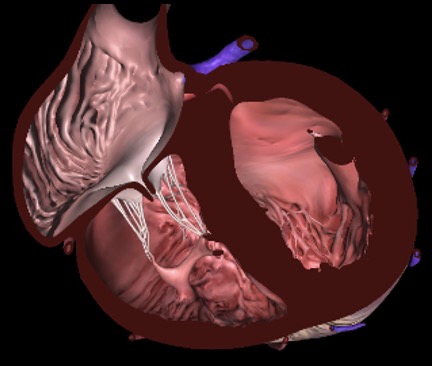
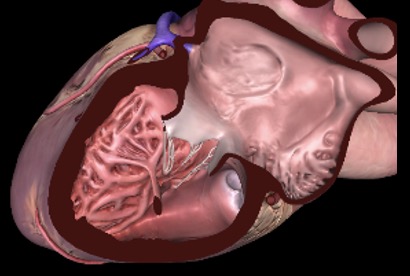
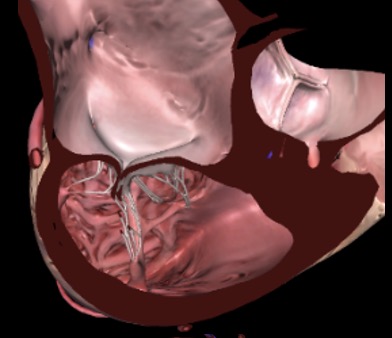
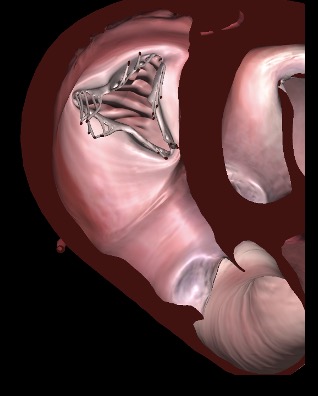
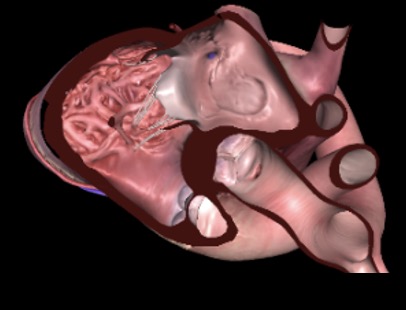
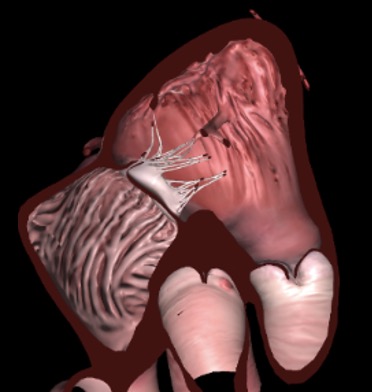
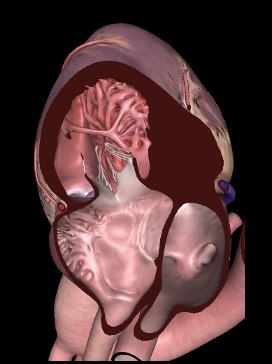
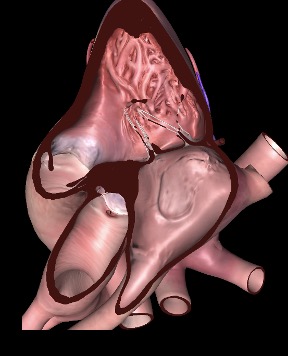
eFigure 18.17
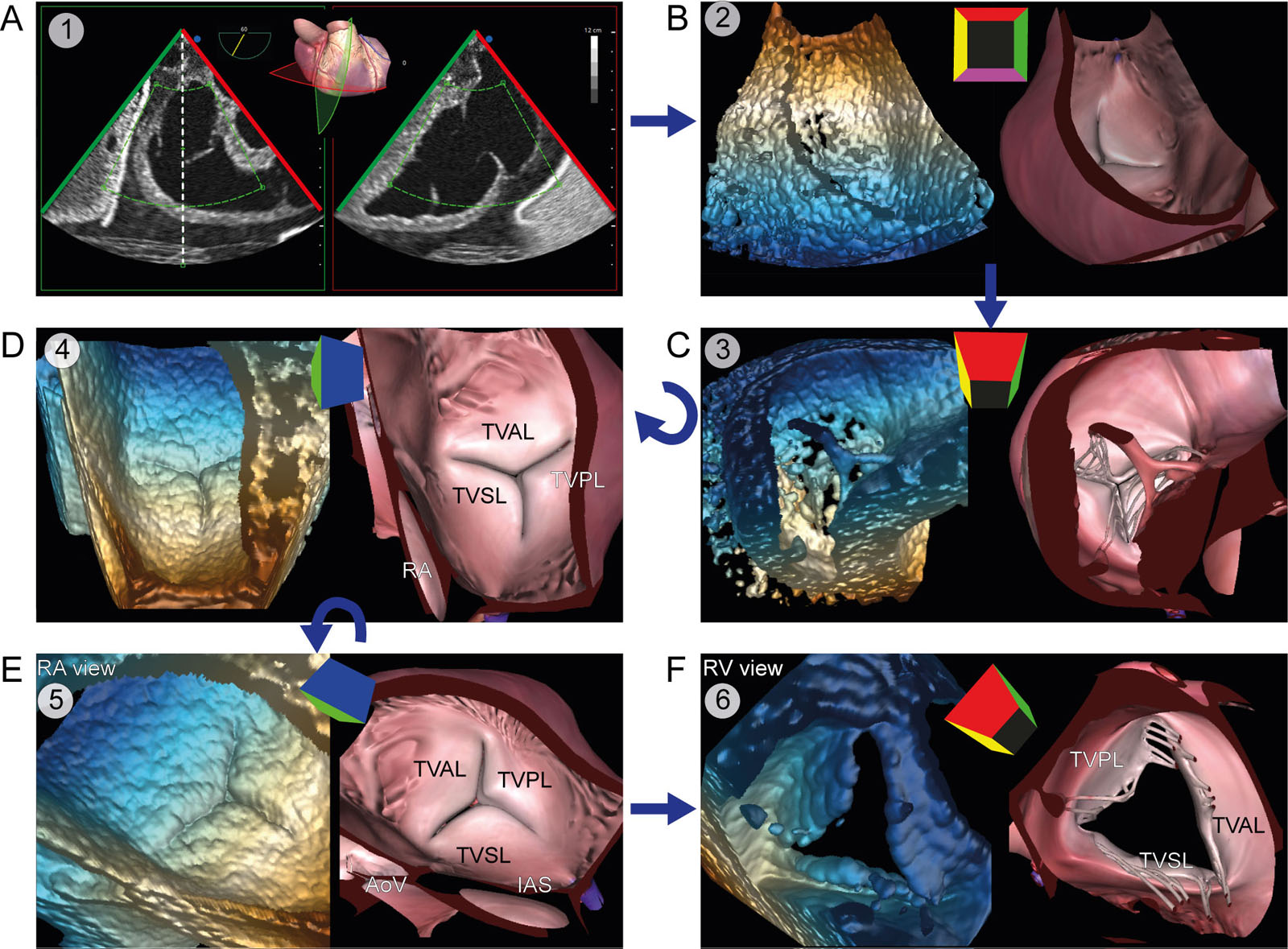
TV 3D zoom acquisition. (A) 3D zoom acquisition should include all three TV leaflets, the TA, and part of the AoV. (B) The acquired 3D frustrum undergoes (C) rotation to (D) display the TV from the RA perspective. (E) Rotation of the RA perspective displays the TV in the surgeon’s orientation. (F) A 180° rotation allows the visualization of an RV view of the TV. Abbreviations: 3D, three-dimensional, AoV, aortic valve; IAS, interatrial septum; RA, right atrium; RV, right ventricle; TA, tricuspid annulus; TV, tricuspid valve; TVAL. Tricuspid valve anterior leaflet; TVPL, tricuspid valve posterior leaflet; TVSL, tricuspid valve septal leaflet.
eFigure 18.26
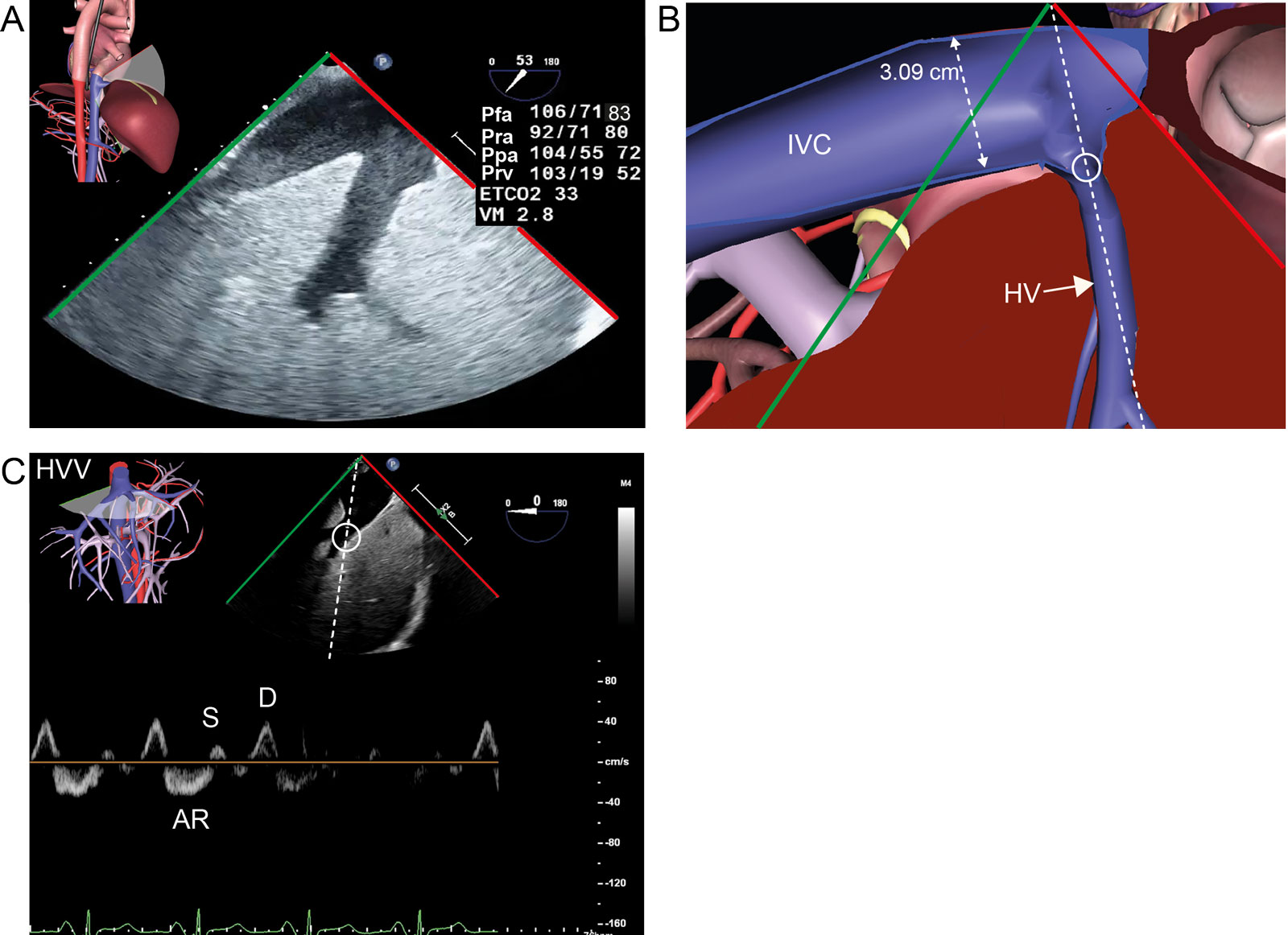
Quantification of TR severity. This is a 76-year-old patient with a history of severe MR. (A,B) TGAUS longitudinal IVC view shows a dilated IVC. (C) The HVV PWD interrogation has systolic blunting with a smaller S compared to D and pronounced AR. TR was moderate in this case. Abbreviations: AR, atrial reversal HVV; D, diastolic HVV; ETCO2, end-tidal CO2; HV, hepatic vein; HVV, hepatic vein velocity; IVC, inferior vena cava; MR, mitral regurgitation; MV, minute ventilation; Pfa, femoral arterial pressure; Ppa, pulmonary artery pressure; Pra, right atrial pressure; Prv, right ventricular pressure; PWD, pulsed-wave Doppler; S, systolic HVV; TGAUS, transgastric abdominal ultrasound; TR, tricuspid regurgitation.
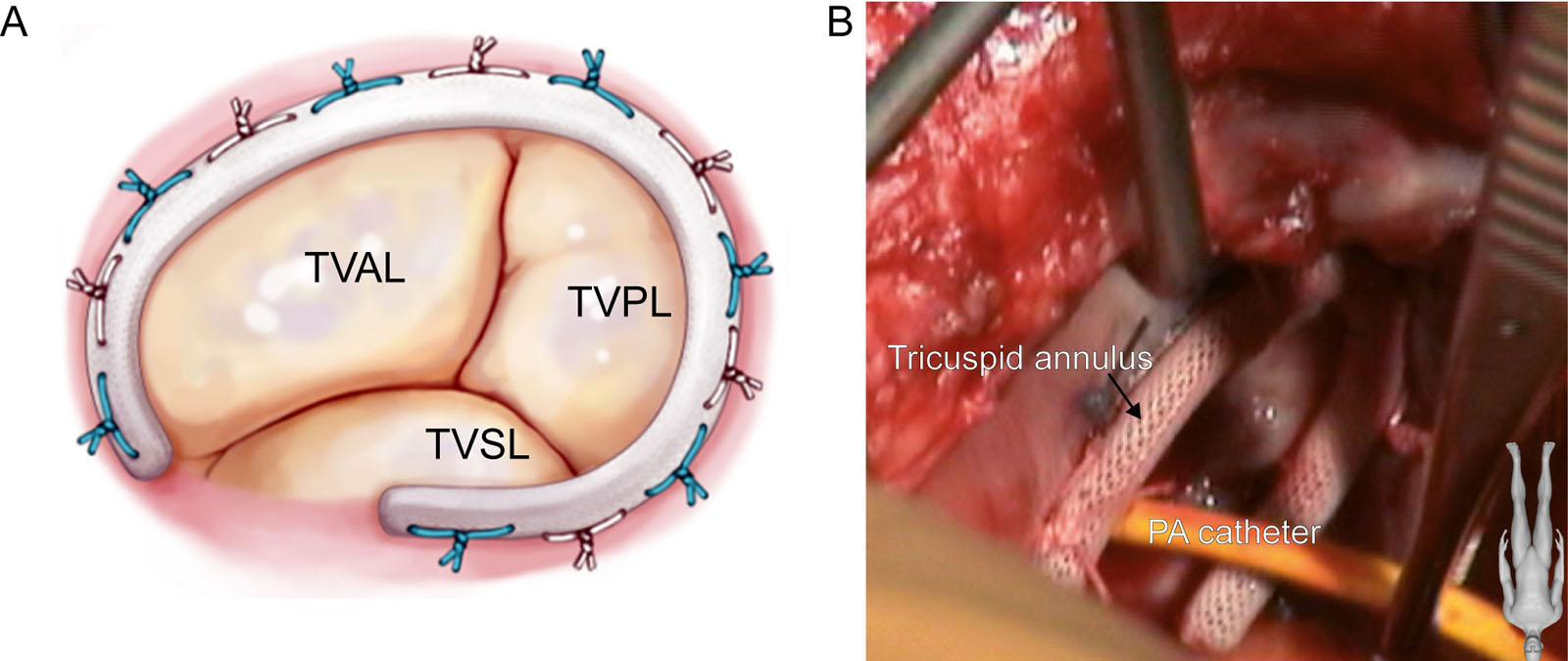
eFigure 18.32
Annuloplasty ring. This is an Edwards® M3C tricuspid annuloplasty ring during implantation in (A) diagram of the TV and (B) an intraoperative photo from the RA. Abbreviations: PA, pulmonary artery; RA, right atrium; TV, tricuspid valve; TVAL, tricuspid valve anterior leaflet, TVPL, tricuspid valve posterior leaflet, TVSL, tricuspid valve septal leaflet.
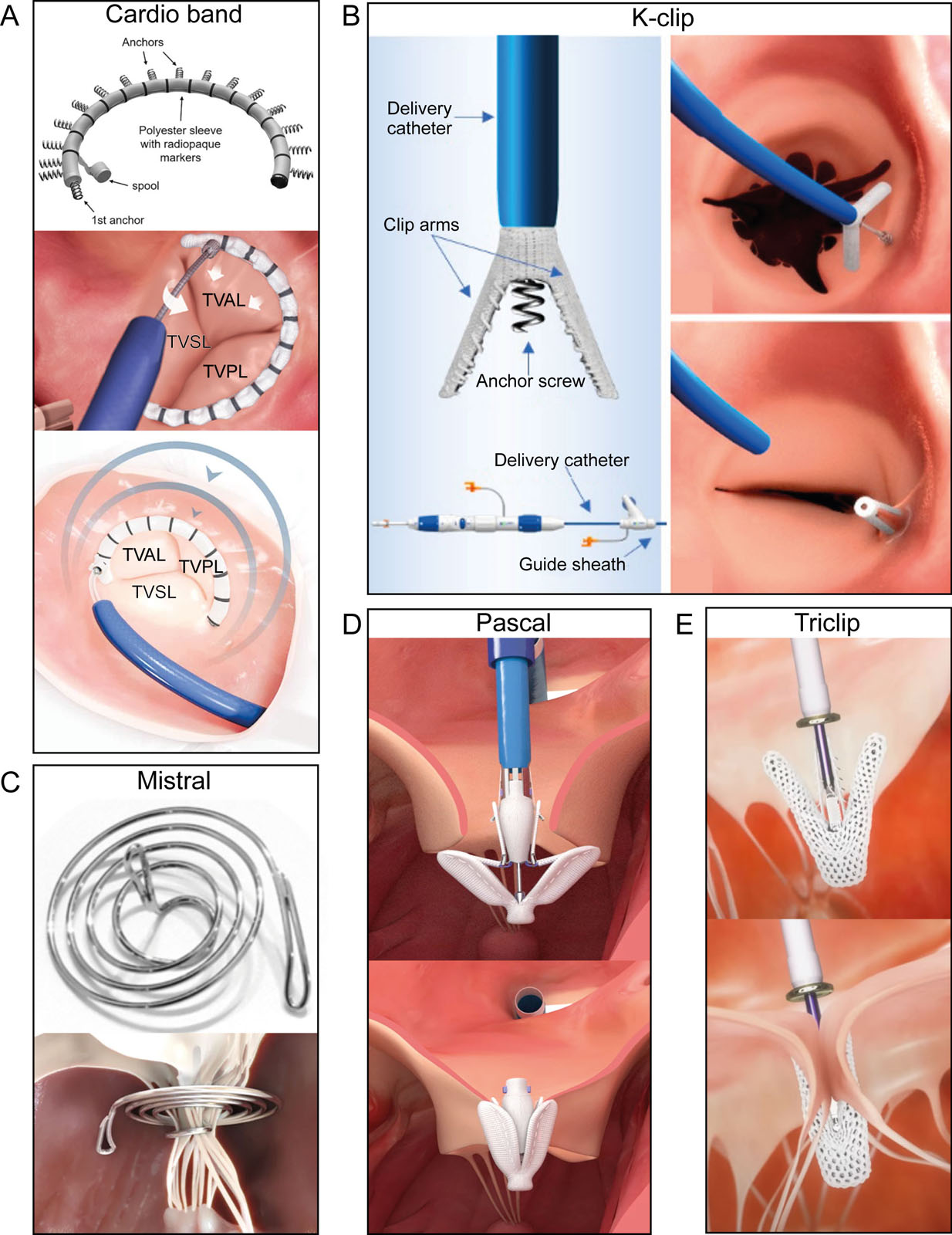
eFigure 18.36
Transcatheter TV repair systems. These are examples of transcatheter TV repair systems, including annuloplasty devices such as the (A) Cardioband (Edwards Lifesciences, Irvine CA, USA) and (B) K-ClipTM (Huihe Co, China)82; subvalvular chordae tendinae approximation devices like the (C) Mistral (Mitralix, Israël) and clip devices (D) Pascal (Edwards Lifesciences, Irvine CA, USA)83 and (E) Triclip (Abbott Vascular, Santa Clara, CA, USA). Abbreviations: TV,tricuspid valve; TVAL, tricuspid valve anterior leaflet; TVPL, tricuspid valve posterior leaflet; TVSL, tricuspid valve septal leaflet.
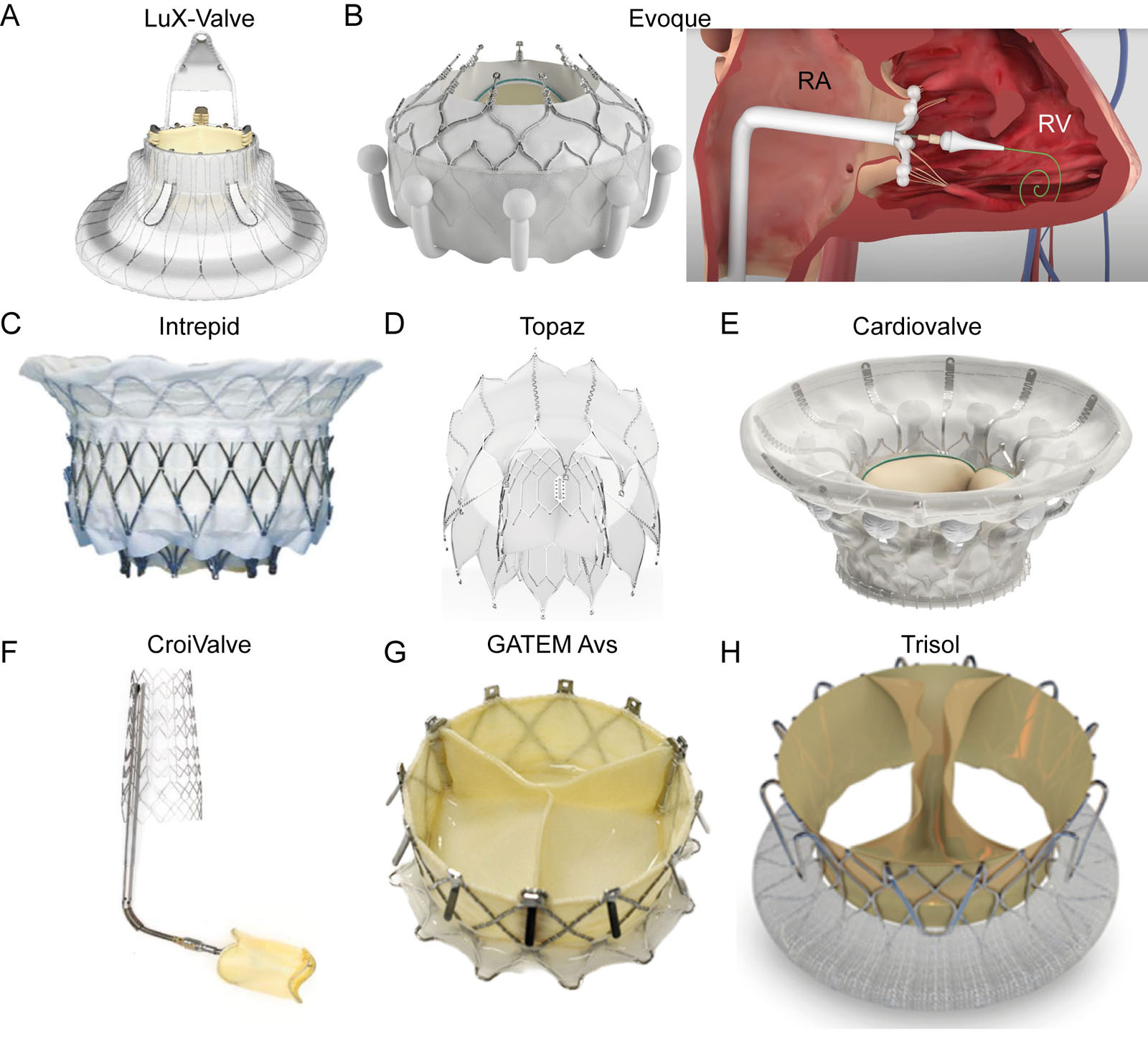
eFigure 18.37
Transcatheter TV orthotopic bioprosthesis. These valves require transfemoral access for implantation, including the (A) LuX-Valve (Jenscare Scientific Co, Ningbo, PRC)84, (B) EVOQUE (Edwards Lifesciences, Irvine, CA, USA), (C) Intrepid (Medtronic, Minneapolis, MN USA), (D) Topaz (TRiCares GmbH, Munich, Germany) and (E) Cardiovalve (Venus Medtech, Hangzhou, PRC) These valves require transjugular access for implantation, including the (F) Duo tricuspid coaptation valve system (CroiValve, Dublin, Ireland)55, (G) GATETM Avs–atrioventricular valved stent (NaviGate Cardiac Structures Inc., Lake Forest, CA, USA) and the (H) Trisol (Trisol Medical, Yokneam, Israel). Abbreviations: RA, right atrium; RV, right ventricle; TV, tricuspid valve.
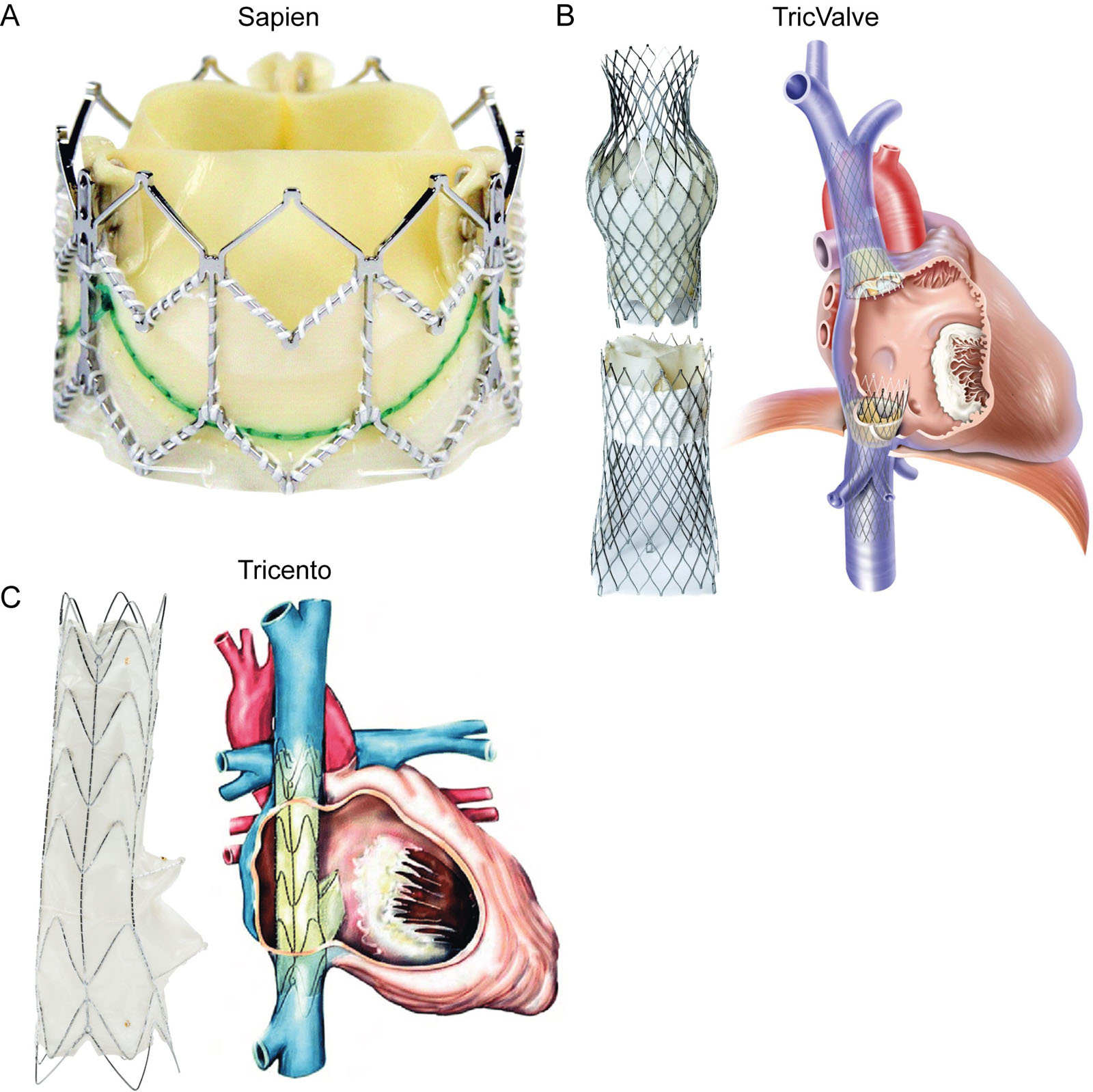
eFigure 18.38
Transcatheter heterotopic bioprosthesis for TR. These are examples of bioprosthetic valves implanted into the IVC and SVC to treat severe TR, including the (A) Sapien XT–Sapien 3 IVC or bicaval IVC+SVC implants (Edwards Lifesciences, Irvine, CA USA). (B) TricValveR Transcatheter bicaval valves system (P+F Products + Features, Vienna, Austria. (C) Tricento (New Valve Technology NVT GmbH, Hechingen, Germany). Abbreviations : IVC, inferior vena cava; SVC, superior vena cava; TR, tricuspid regurgitation.
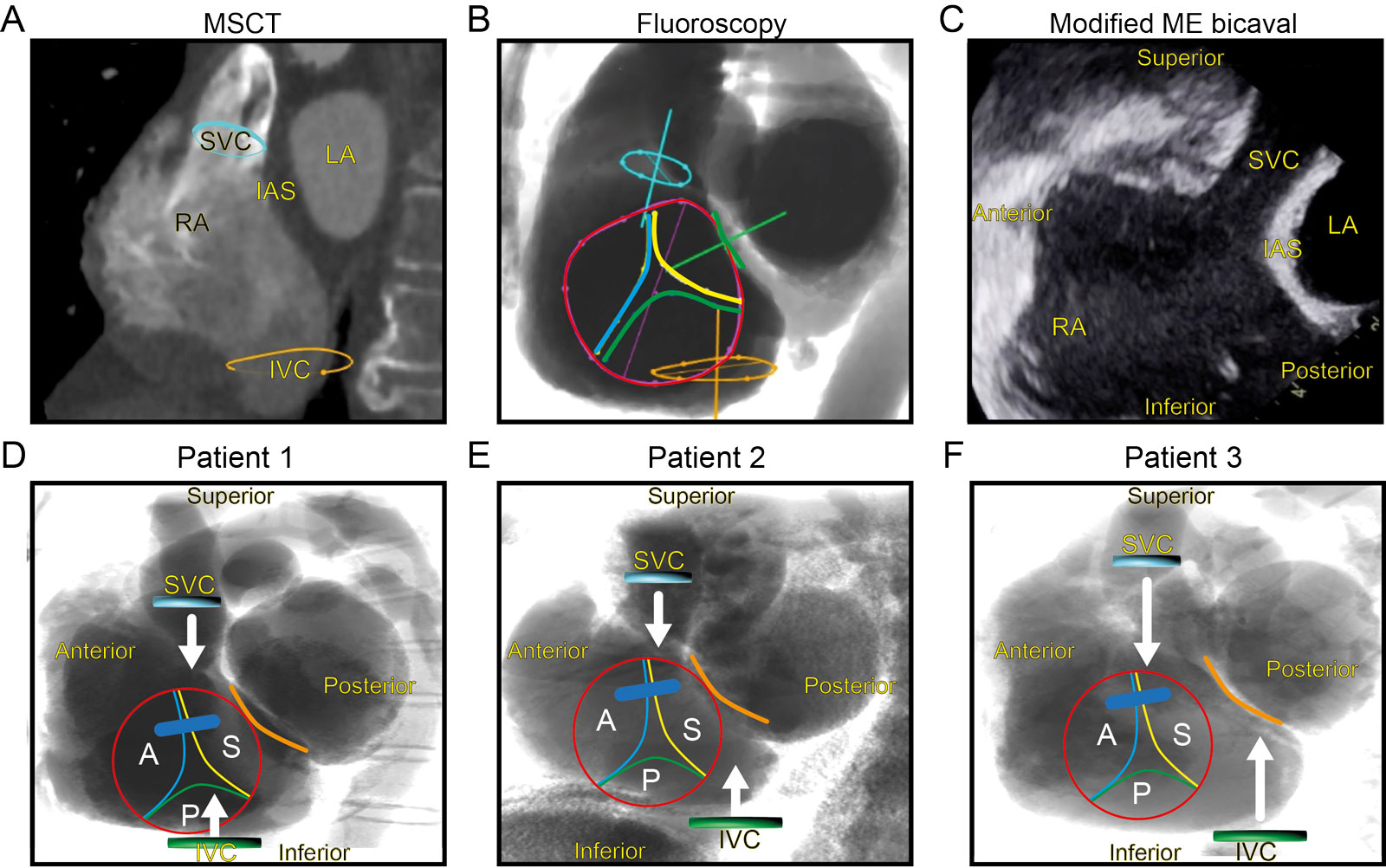
eFigure 18.40
Preprocedural imaging for tricuspid intervention. This is the (A) preprocedural cardiac CTA and (B) corresponding fluoroscopic view with projection of the TV leaflets. (C) From the corresponding TEE bicaval view, the image display would need counterclockwise rotation and then left-right inversion to match the fluoroscopic view. (D) The lower row shows similar fluoroscopic LAO caudal one-chamber en-face views of the TV in three different patients, revealing a variable degree of TV position offset (red circle) from the SVC (blue) and the IVC (green) orifices. This explains how the alignment between the SVC, IVC and TV varies between patients. In patient #3, the catheter arriving from the IVC will encounter the septum. Abbreviations: A, anterior; CTA, computed tomography angiography; IAS, interatrial septum; IVC, inferior vena cava; LA, left atrium; LAO, left anterior oblique; ME, mid-esophageal; MSCT, multi-slice computed tomography; P, posterior; RA, right atrium; S, septal; SVC, superior vena cava; TEE, transesophageal echocardiography; TV, tricuspid valve.
Videos
Chapter 18 Fig01A
Chapter 18 Fig01B
Chapter 18 Fig05CD
Chapter 18 Fig06A
Chapter 18 Fig07A
Chapter 18 Fig08A
Chapter 18 Fig09A
Chapter 18 Fig10A
Chapter 18 Fig11A
Chapter 18 Fig11D
Chapter 18 Fig12A
Chapter 18 Fig12C
Chapter 18 Fig13A
Chapter 18 Fig13F
Chapter 18 Fig14A
Chapter 18 Fig15A
Chapter 18 Fig16A1
Chapter 18 Fig16A2
Chapter 18 Fig16A3
Chapter 18 Fig16B1
Chapter 18 Fig16B2
Chapter 18 Fig16B3
Chapter 18 Fig16C1
Chapter 18 Fig16C2
Chapter 18 Fig16D
Chapter 18 Fig16E1
Chapter 18 Fig16E2
Chapter 18 Fig16E3
Chapter 18 Fig17ABCDEF
Chapter 18 Fig18A
Chapter 18 Fig18C
Chapter 18 Fig19A
Chapter 18 Fig20AB
Chapter 18 Fig20C
Chapter 18 Fig21A
Chapter 18 Fig21B
Chapter 18 Fig22A
Chapter 18 Fig22C
Chapter 18 Fig22EF
Chapter 18 Fig23AD
Chapter 18 Fig24C
Chapter 18 Fig24DE
Chapter 18 Fig26A
Chapter 18 Fig27A
Chapter 18 Fig27B
Chapter 18 Fig27D
Chapter 18 Fig28A
Chapter 18 Fig32B
Chapter 18 Fig34A
Chapter 18 Fig34B
Chapter 18 Fig34E
Chapter 18 Fig35A
Chapter 18 Fig35B
Chapter 18 Fig35D
Chapter 18 Fig35E
Chapter 18 Fig36A
Chapter 18 Fig36C
Chapter 18 Fig36D
Chapter 18 Fig36E
Chapter 18 Fig37B
Chapter 18 Fig37D
Chapter 18 Fig37E
Chapter 18 Fig37F
Chapter 18 Fig37H
Chapter 18 Fig38B
Chapter 18 Fig39A
Chapter 18 Fig39C
Chapter 18 Fig39E
Chapter 18 Fig39FG
Chapter 18 Fig41A
Chapter 18 Fig41D
Chapter 18 Fig42A
Chapter 18 Fig42C
Chapter 18 Fig43A
Chapter 18 Fig44A
Chapter 18 Fig45A
Chapter 18 Fig46A
Chapter 18 Fig46D
Tables
eTable 18.1 TEE views for assessing the tricuspid valve
TEE View |
Icon |
View-Technique |
Utility/disadvantages |
 |
ME 4C RV focus |
|
|
 |
ME RV Inflow-Outflow |
|
|
 |
ME Modified Bicaval TV |
|
|
 |
DE 2C TV |
|
|
 |
DE Coronary sinus LAX |
|
|
 |
DE RV inflow-outflow |
|
|
 |
TG RV basal |
|
|
 |
TG RV inflow |
|
|
 |
TG RV Inflow outflow |
|
|
 |
DTG RV inflow |
|
|
 |
DTG RV inflow-outflow |
|