Figures
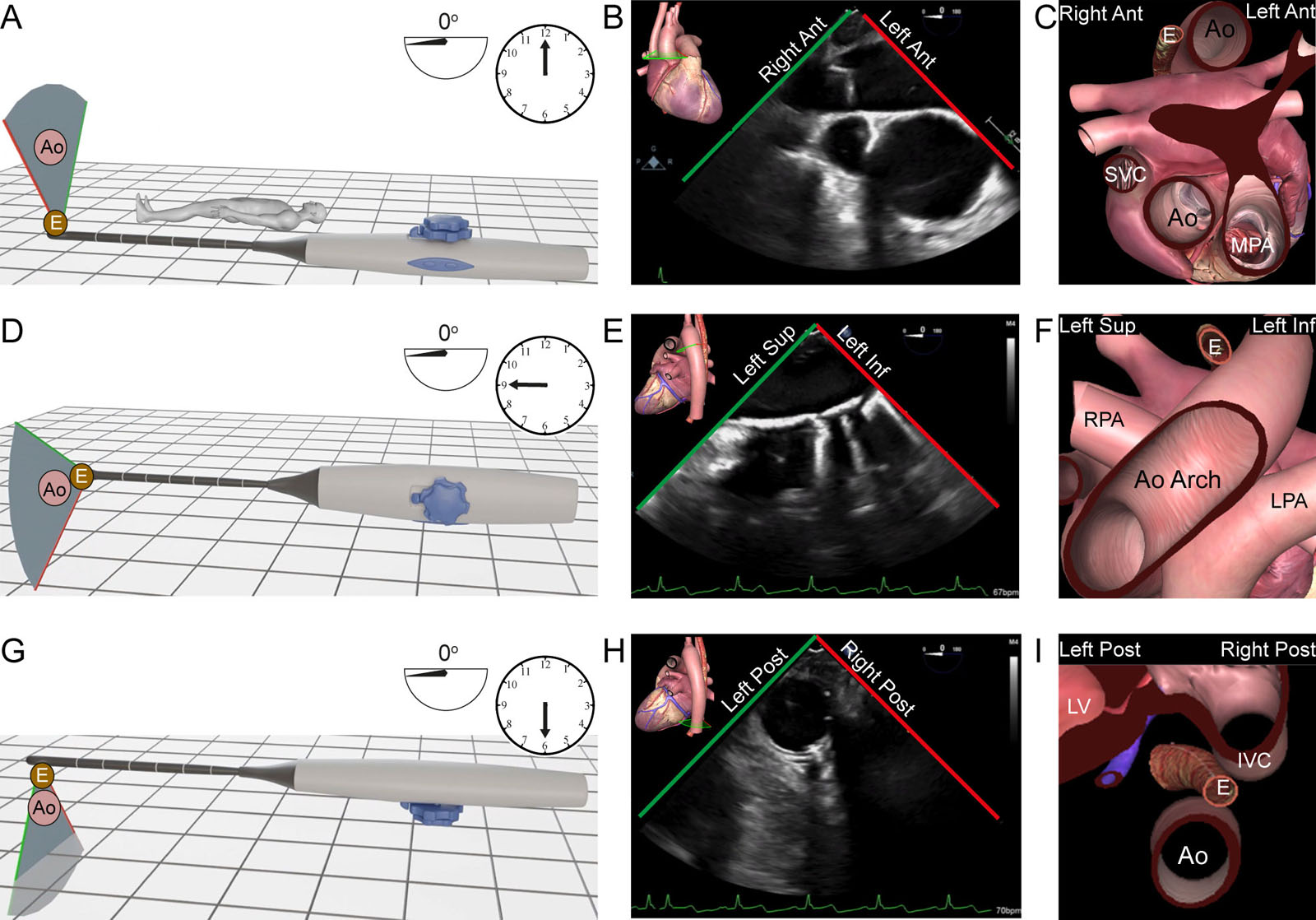
eFigure 23.6
TEE thoracic aorta examination. These diagrams show the relationship between the TEE probe and the structures displayed during the thoracic aorta examination. (A-D) ME Asc Ao SAX view. In this position, the dual rotating knob position is anterior at 12 o’clock and the US beam is at 0°. In the 2D image, the right screen (red line) has the left anterior anatomic structures like the MPA and the left screen (green line) the right anterior anatomic structures like the SVC. The Ao lies anterior to the esophagus. (E-H) UE aortic arch SAX view. The dual rotating knob position is to the left of the patient at 9 o’clock and the US beam is at 0°. In the 2D image, the right screen (red line) corresponds to the left inferior anatomic structures like the LPA and the left screen (green line) to the left superior anatomic structures like the RPA. (I-L) DE descending aorta SAX view. The dual rotating knob position is in the back of the patient, posteriorly at 6 o’clock and the US beam is at 0°. In the 2D image, the right screen (red line) corresponds to the right inferior anatomic structures like the IVC and the left screen (green line) to the left inferior anatomic structures like the LV. Abbreviations: 2D, two-dimensional; Ant, anterior; Ao, aorta; Asc Ao, ascending aorta; DE, deep esophageal; E, esophagus; Inf, inferior; IVC, inferior vena cava; LPA, left pulmonary artery; LV, left ventricle; ME, mid-esophageal; MPA, main pulmonary artery; Post, posterior; RPA, right pulmonary artery; SAX, short-axis; Sup, superior; SVC, superior vena cava; UE, upper esophageal; US, ultrasound. Adapted from Denault at al. 71 Artwork courtesy of Hugo Babin.
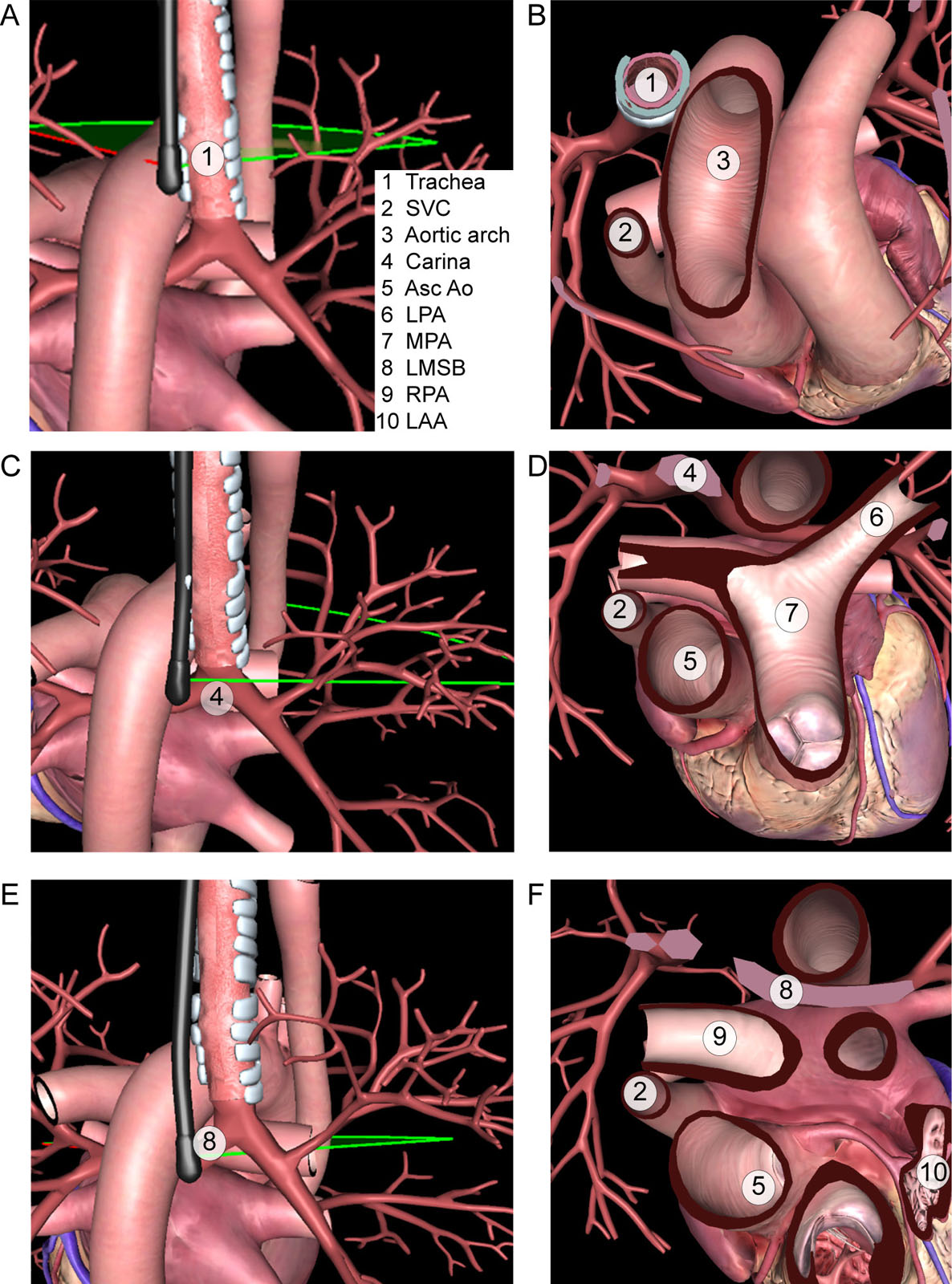
eFigure 23.7
TEE blind spot. Interposition of the trachea (A,B), carina (C,D) and LMSB (E,F) anterior to the TEE probe creates blind areas where several cardiac structures (1 to 7) may not be identified clearly. Abbreviations: Asc Ao, ascending aorta; LAA, left atrial appendage; LMSB, left main stem bronchus; LPA, left pulmonary artery; MPA, main pulmonary artery; RPA, right pulmonary artery; SVC, superior vena cava; TEE, transesophageal echocardiography. Adapted from Sharma et al. 72
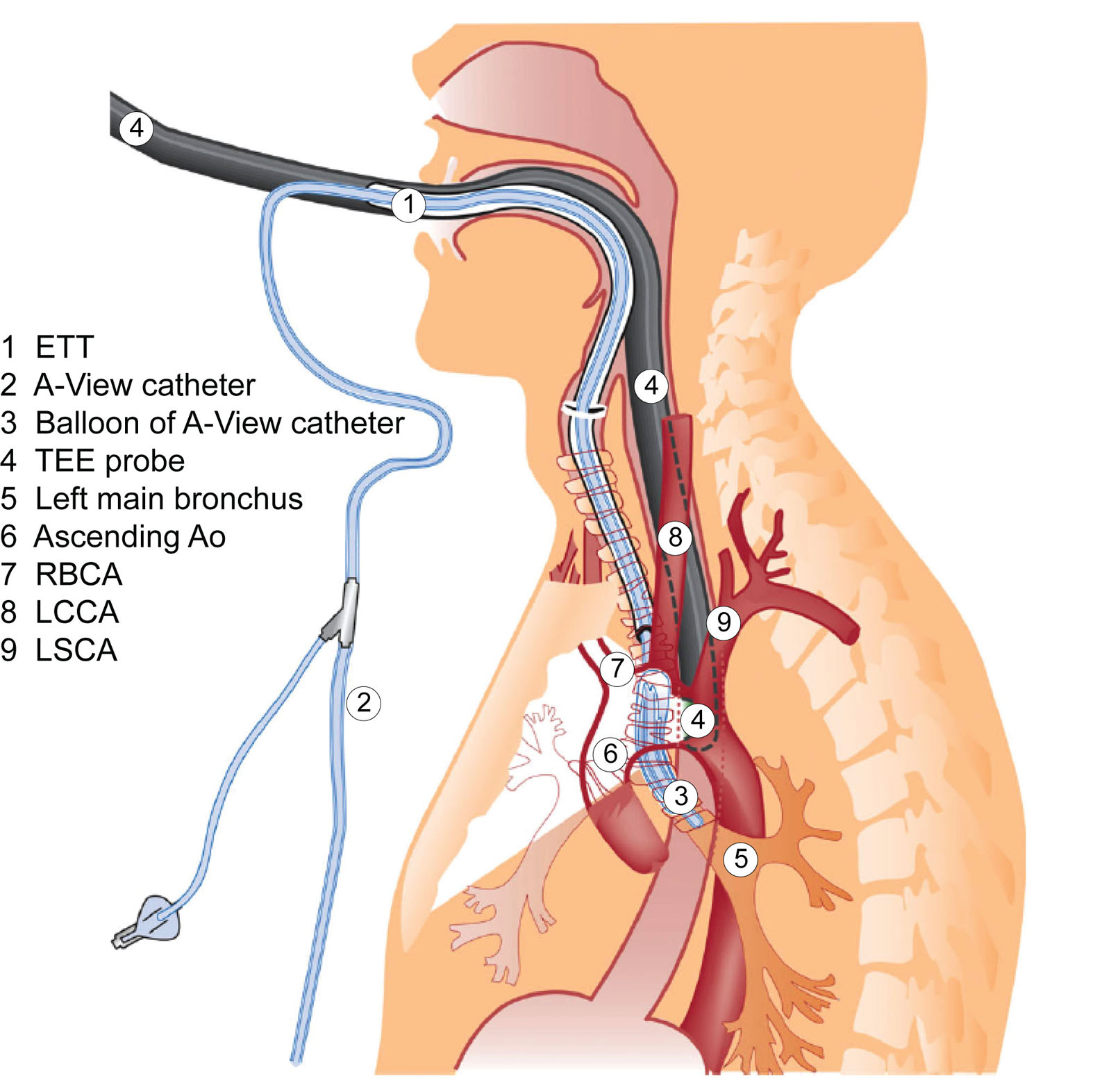
eFigure 23.8
A-View balloon catheter. This sagittal cross-section view illustrates the anatomic relationship of structures with the A-View balloon catheter (DeRoyals, TN, USA), and TEE probe. Abbreviations: Ao, aorta; ETT, endotracheal tube; LCCA, left common carotid artery; LSCA, left subclavian artery; RBCA, right brachiocephalic artery; TEE, transesophageal echocardiography. Source: Adapted with permission from van Zaane et al.10
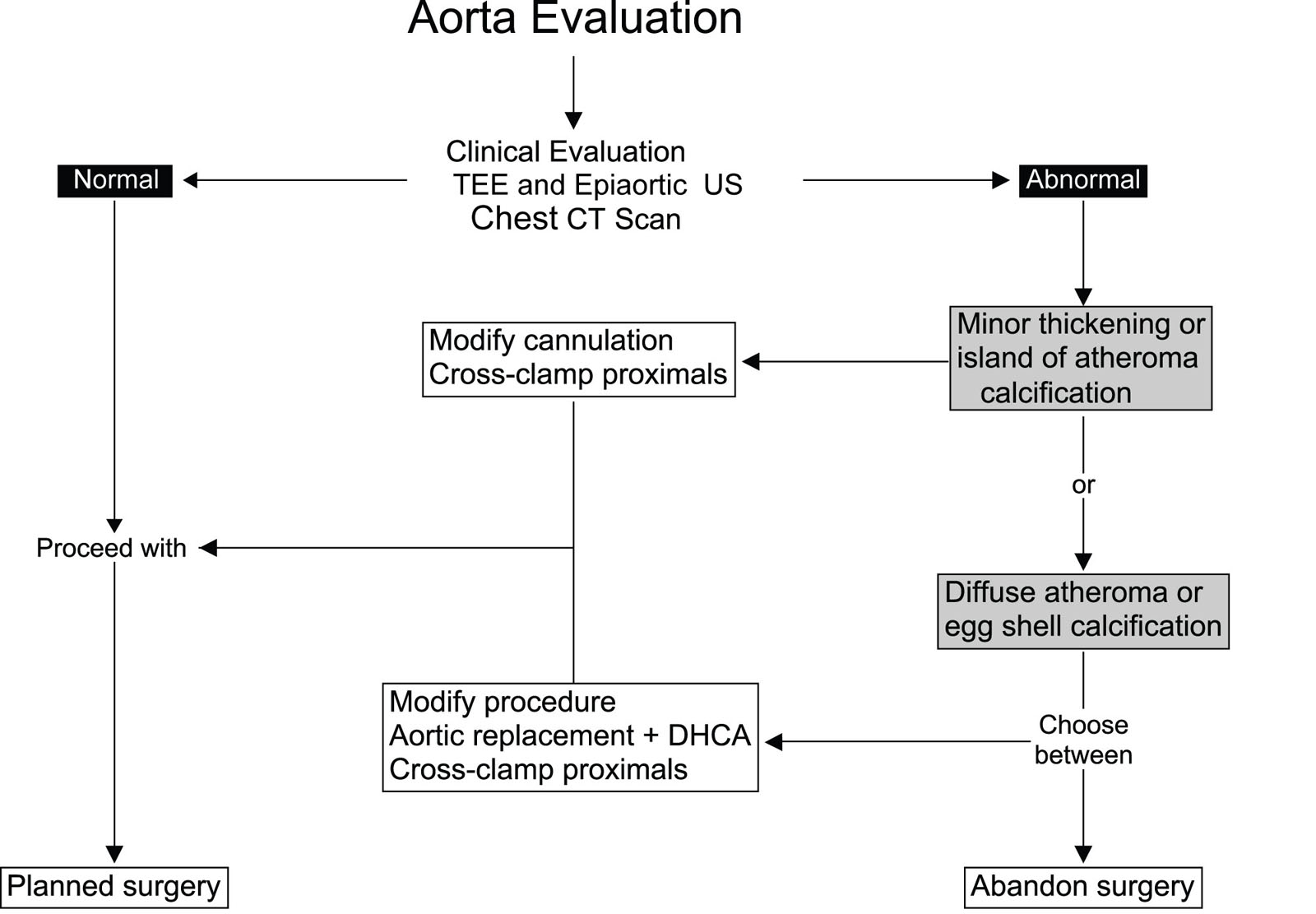
eFigure 23.15
Aortic atheroma algorithm. This algorithm demonstrates the management of Asc Ao atheroma during cardiac surgery. Abbreviations: Asc Ao, ascending aorta; CT, computed tomography; DHCA, deep hypothermic cardiac arrest; TEE, transesophageal echocardiography; US, ultrasound.
eFigure 23.17
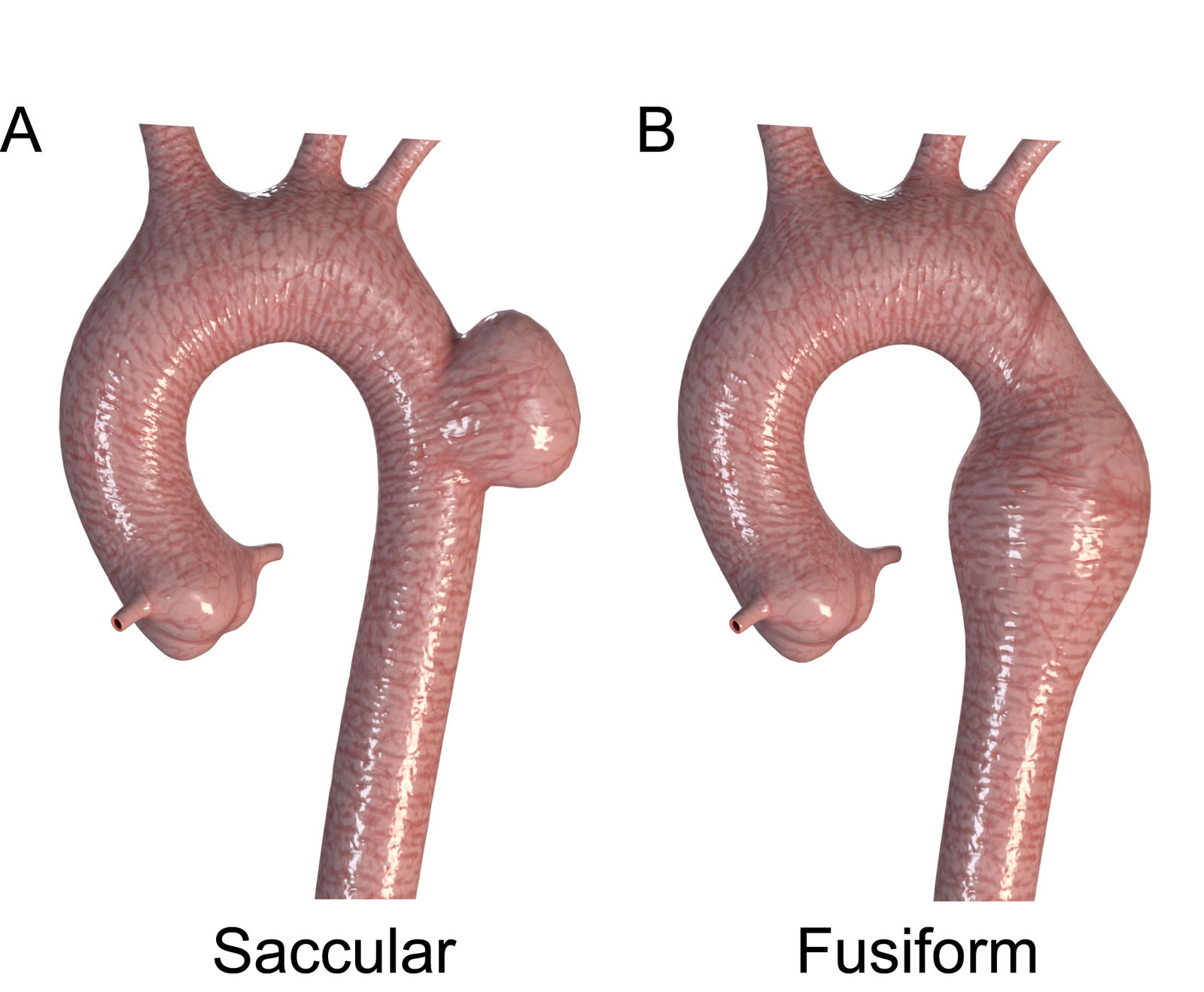
Aneurysm morphology. (A,B) These diagrams illustrate the two morphologic types of aortic aneurysms, (A) saccular and (B) fusiform. Adapted from Isselbacher et al.68
eFigure 23.19
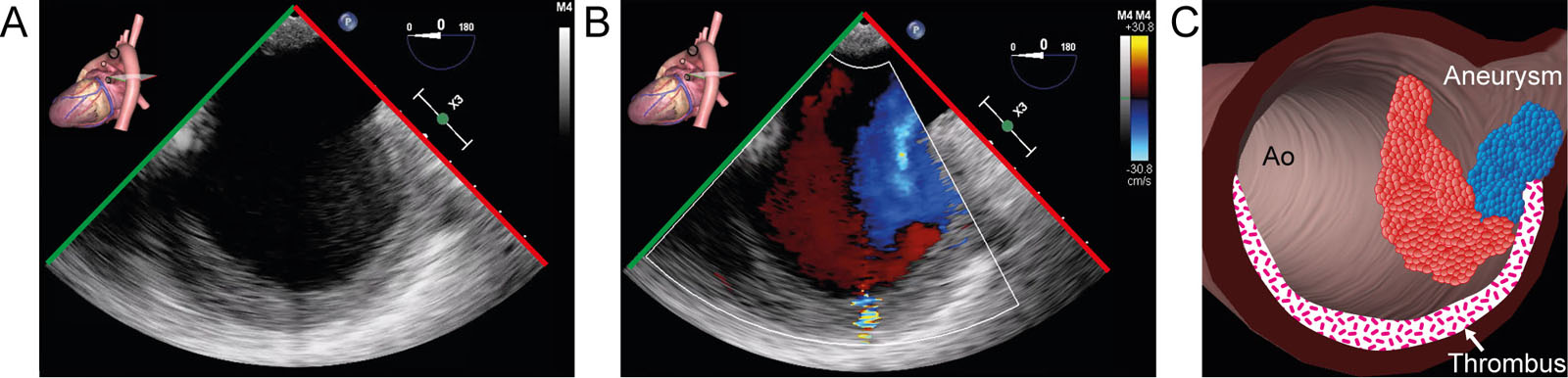
Saccular aneurysm. (A-C) Desc Ao SAX view with CFI shows a saccular aneurysm with a thrombus. Abbreviations: Ao, aorta; CFI, color flow imaging; Desc Ao, descending aorta; SAX, short-axis.
eFigure 23.24
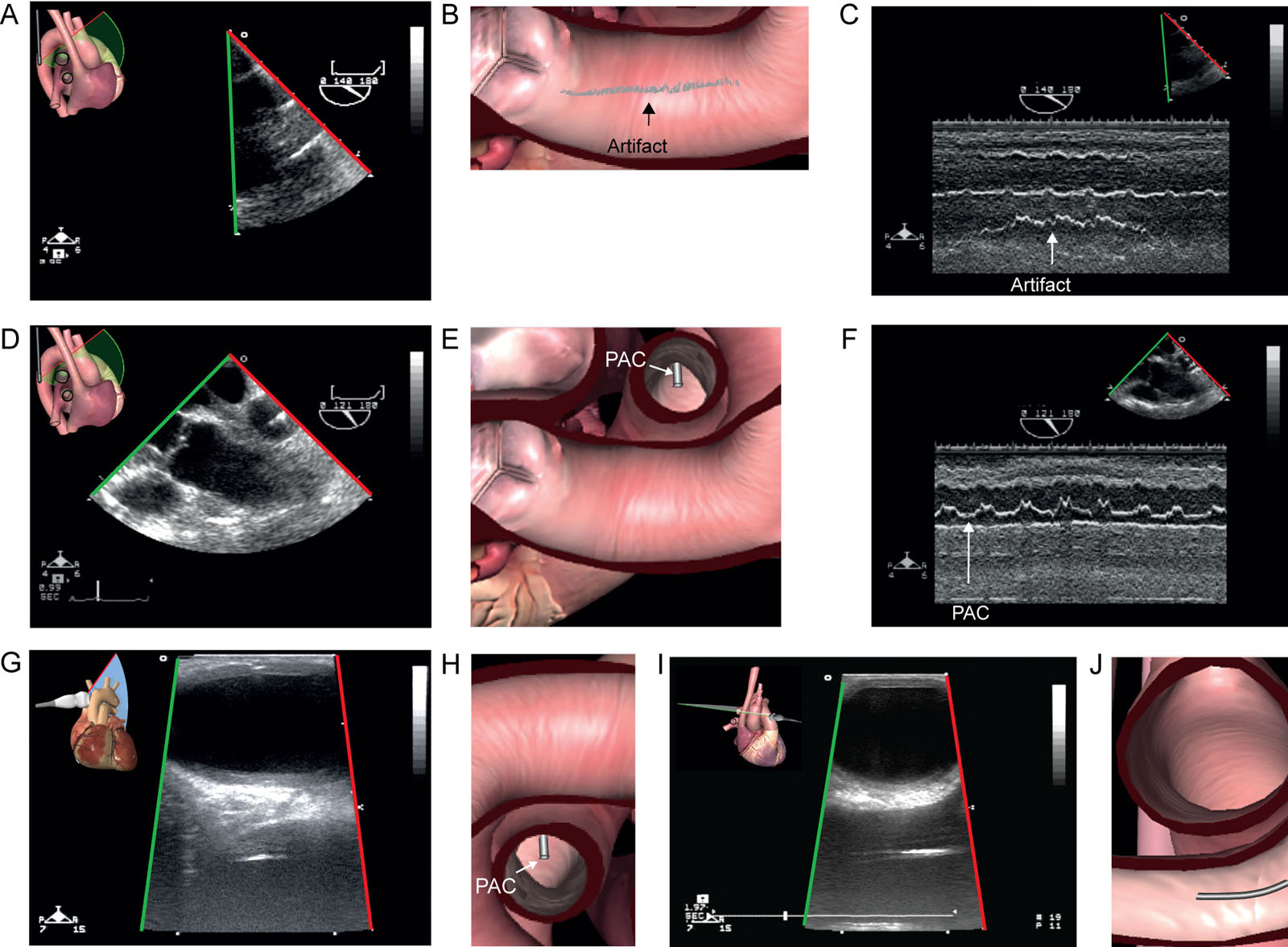
Pseudo-aortic dissection. A 57-year-old man undergoing coronary bypass surgery experiences problematic aortic cannula insertion, giving rise to suspicion of an aortic dissection. (A, B) ME Ao LAX view shows a mobile linear shadow suggestive of an intimal flap. (C) Corresponding M-mode of the suspected intimal flap (arrow) below the aortic wall. (D, E) ME Asc Ao LAX shows a PAC in the RPA. (F) On M-mode, the PAC motion (arrow) has an excursion quite like the suspected intimal flap. (G–J) Epiaortic scanning of the ascending Ao in G, H) LAX and (I, J) SAX fails to show a dissection flap, excluding an aortic dissection. The linear shadow represents a reverberation artifact in the aorta from the PAC in the RPA. Abbreviations: Ao, aorta; Asc Ao, ascending aorta; LAX, long-axis; ME, mid-esophageal; PAC, pulmonary artery catheter; RPA, right pulmonary artery; SAX, short-axis.
eFigure 23.27
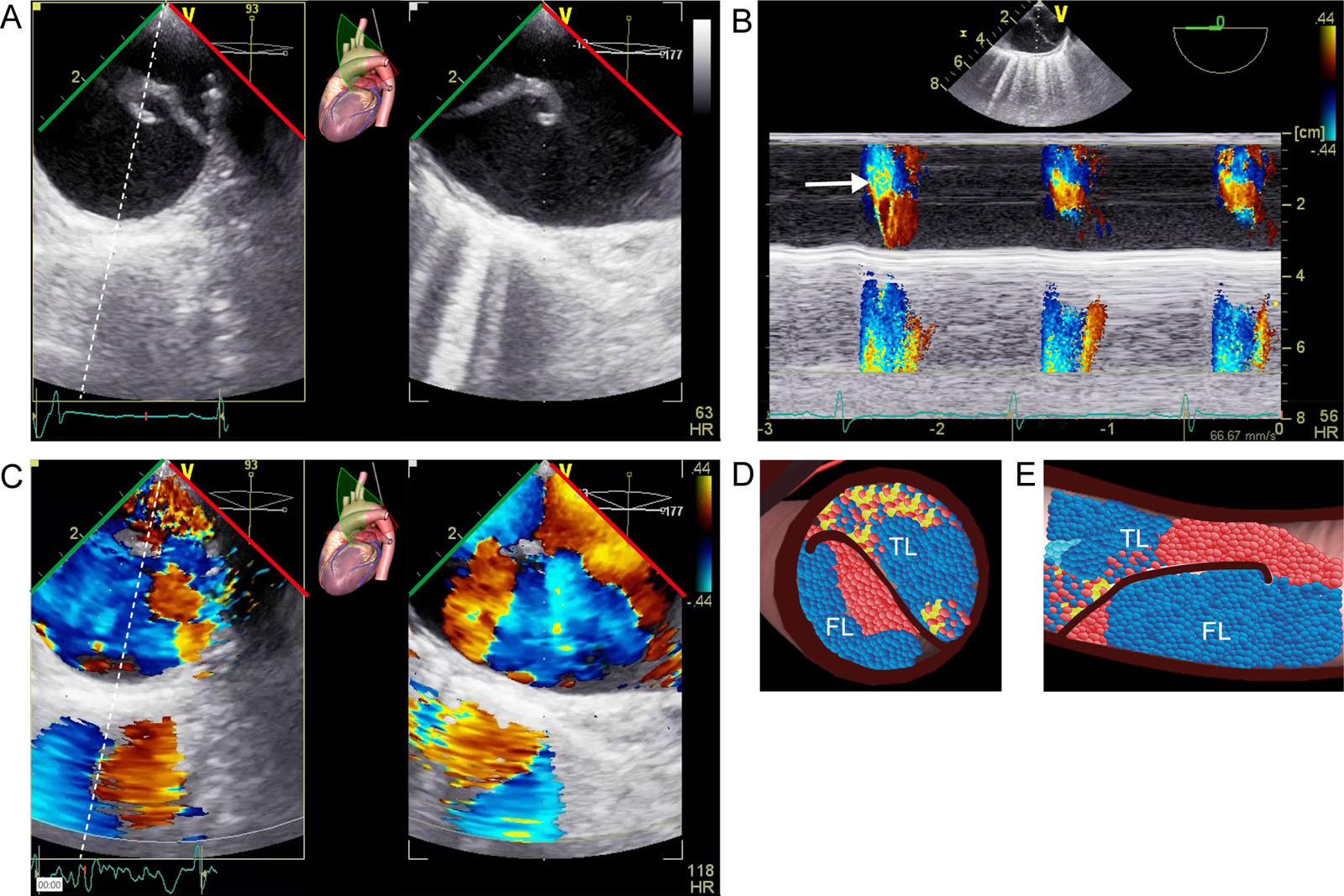
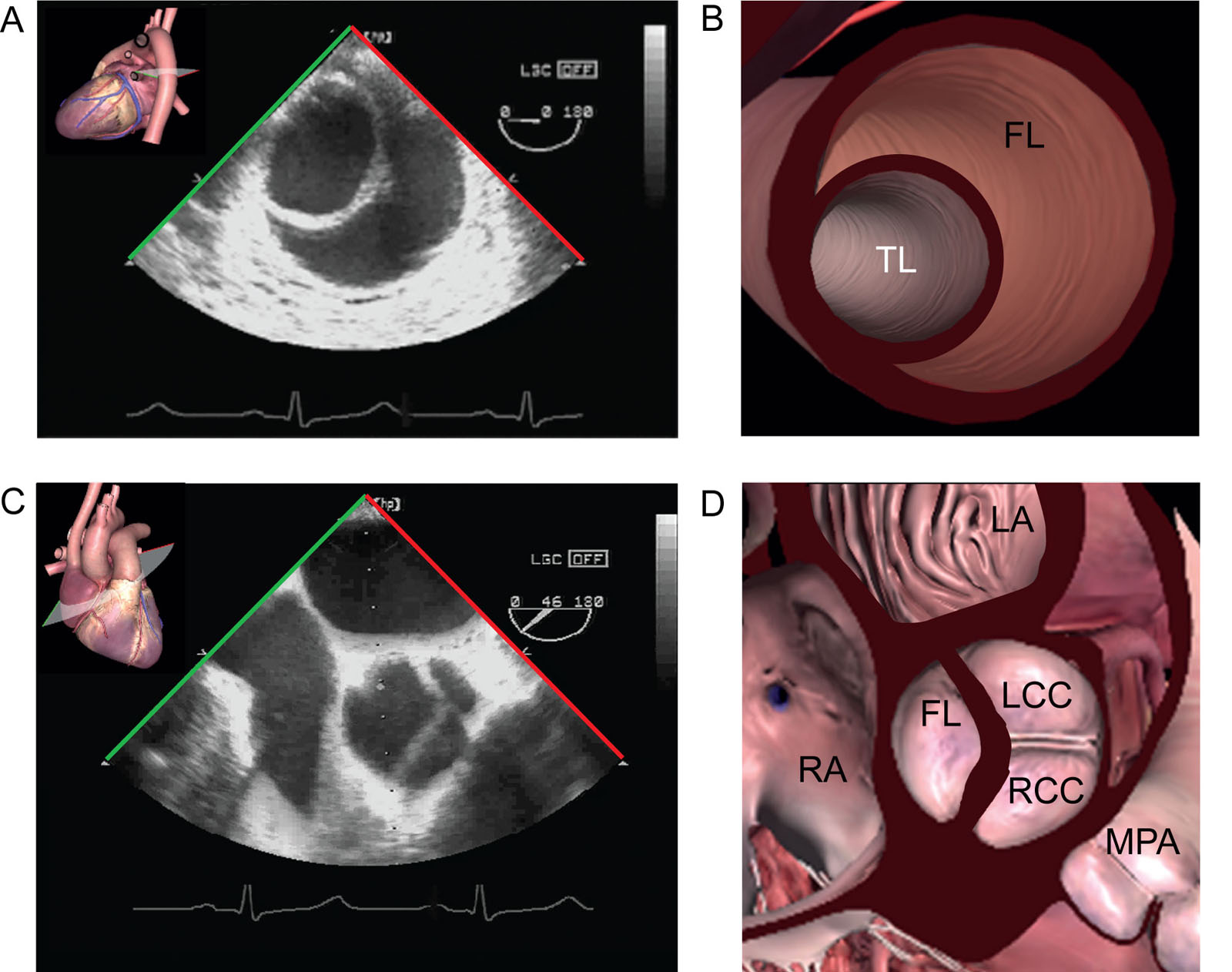
Aortic dissection Stanford type A. (A) Biplane ME Desc Ao SAX view shows the TL has a smaller diameter and is more pulsatile compared with the FL. (B) Color M-mode can help identify the TL where most systolic aliasing occurs versus FL. (C-E) Biplane ME AoV SAX view with CFI shows flow in both the TL and FL. Abbreviations: AoV, aorta valve; CFI, color flow imaging; Desc Ao, descending aorta;FL, false lumen; ME, mid-esophageal; SAX, short-axis; TL, true lumen.
eFigure 23.28
Aortic dissection Stanford type A. (A, B) ME descending aorta SAX view shows the TL has a smaller diameter and is more pulsatile compared with the FL. (C, D) ME AoV SAX view shows a proximal extension of the intimal flap to the level of the sinuses of Valsalva above the AoV. Abbreviations: AoV, aorta valve; FL, false lumen; LA, left atrium; LCC, left coronary cusp; ME, mid-esophageal; MPA, main pulmonary artery; RA, right atrium; RCC, right coronary cusp; SAX, short-axis; TL, true lumen.
eFigure 23.32
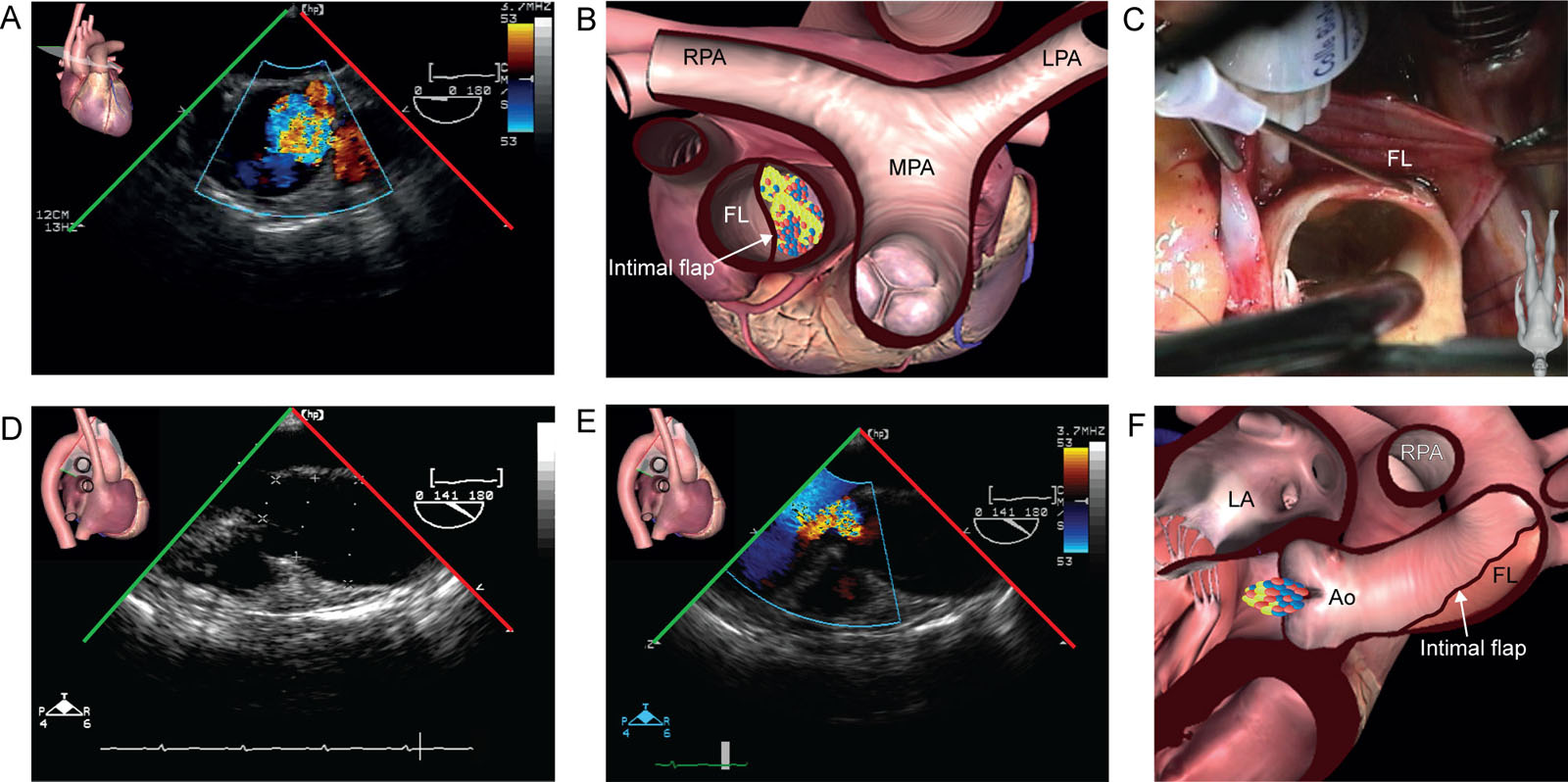
Aortic dissection and AR. This 59-year-old woman experienced sudden excruciating chest pain and a CT scan diagnosed a Stanford type A aortic dissection. (A, B) ME ascending Ao SAX view shows the FL involving the proximal ascending aorta. (C) this is an intraoperative photo of the findings. (D-F) ME AoV LAX views without and with CFI show the dissection was associated with moderate AR. Abbreviations: Ao, aorta; AR, aortic regurgitation; AoV, aortic valve; CFI, color flow imaging; CT, computed tomography; FL, false lumen; LA, left atrium; LAX, long-axis; LPA, left pulmonary artery; ME, mid-esophageal; MPA, main pulmonary artery; RPA, right pulmonary artery; SAX, short-axis. Source: Photo C courtesy of Drs. Nicolas Noiseux and Raymond Cartier.
eFigure 23.34
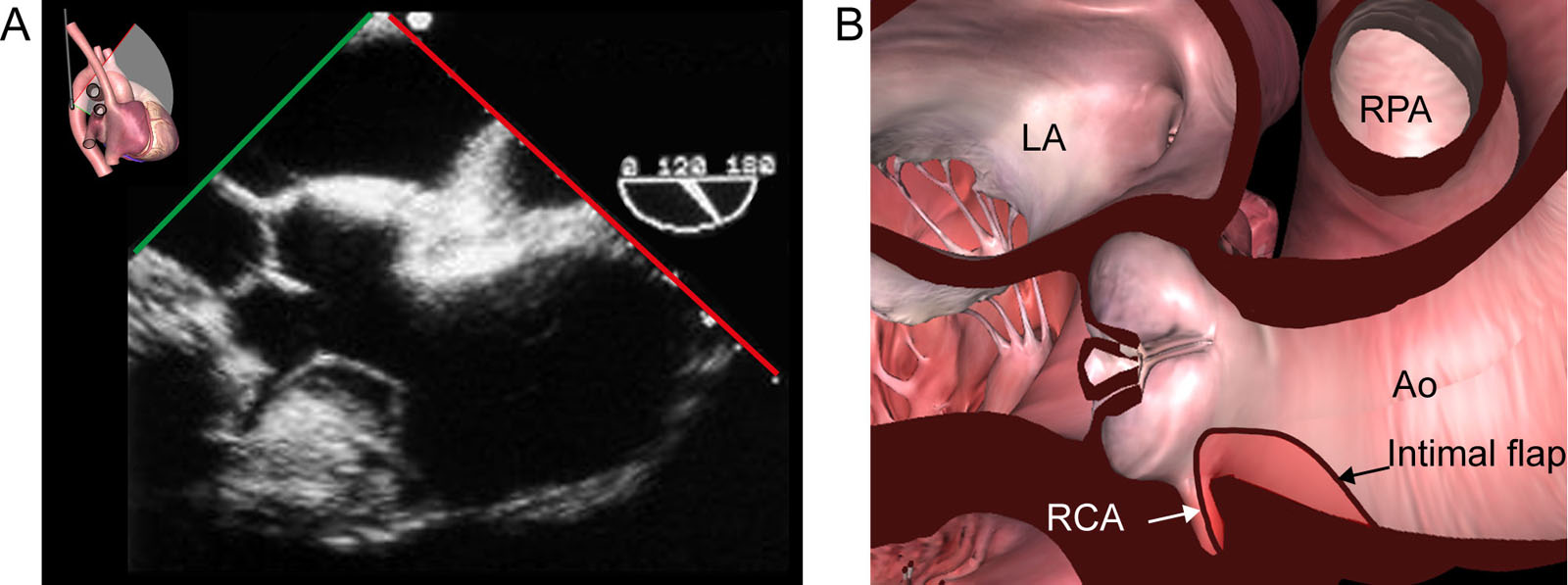
Dissection and coronary perfusion. (A, B) ME Asc Ao LAX view from a patient with type A aortic dissection illustrates the dissection flap (arrow) entering the ostium of the RCA. Abbreviations: Ao, aorta; Asc Ao, ascending aorta; LA, left atrium; LAX, long-axis; ME, mid-esophageal; RCA, right coronary artery; RPA, right pulmonary artery. With the permission of Goldstein et al. 65
eFigure 23.36
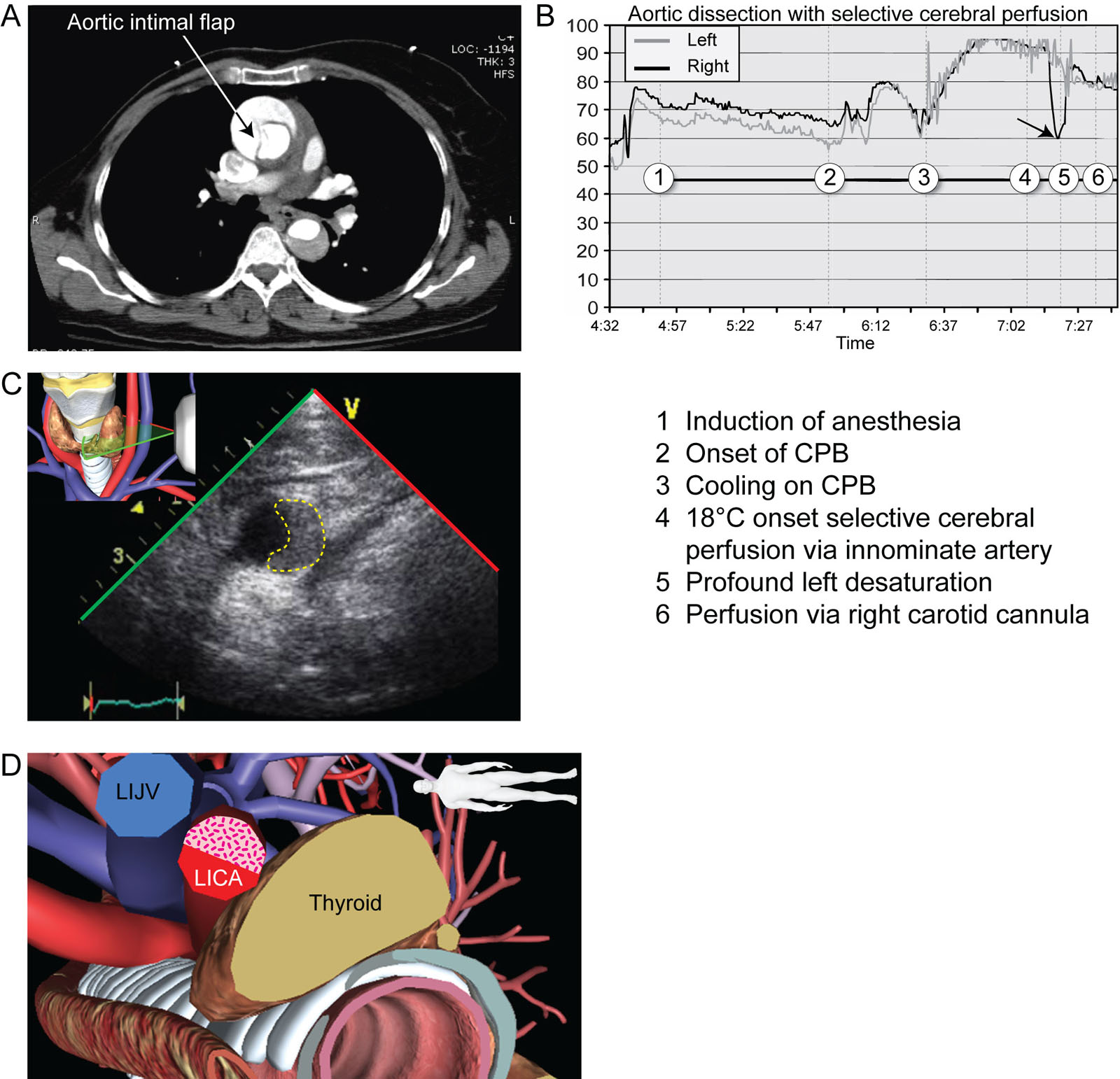
Aortic dissection and cerebral perfusion. (A) Axial slice of a CT angiogram shows dissection of the Asc Ao (arrow) extending to the Desc Ao. (B) Intraoperative brain oximetry monitoring after selective unilateral cerebral perfusion via the innominate artery shows an immediate profound decrease in right rSO2 (arrow point #5). This required the establishment of perfusion via a right carotid artery cannula with the restoration of right rSO2. This unilateral desaturation is most probably because of an incomplete circle of Willis. (C, D) Surface transverse scan of the LICA shows partial occlusion from the extension of a Stanford type A aortic dissection. Note the partial occlusion of the LICA. Abbreviations: Asc Ao, ascending aorta; CPB, cardiopulmonary bypass; CT, computed tomography; Desc Ao, descending aorta; LICA, left internal carotid artery; LIJV, left internal jugular vein; rSO2, regional oxygen saturation.
eFigure 23.37
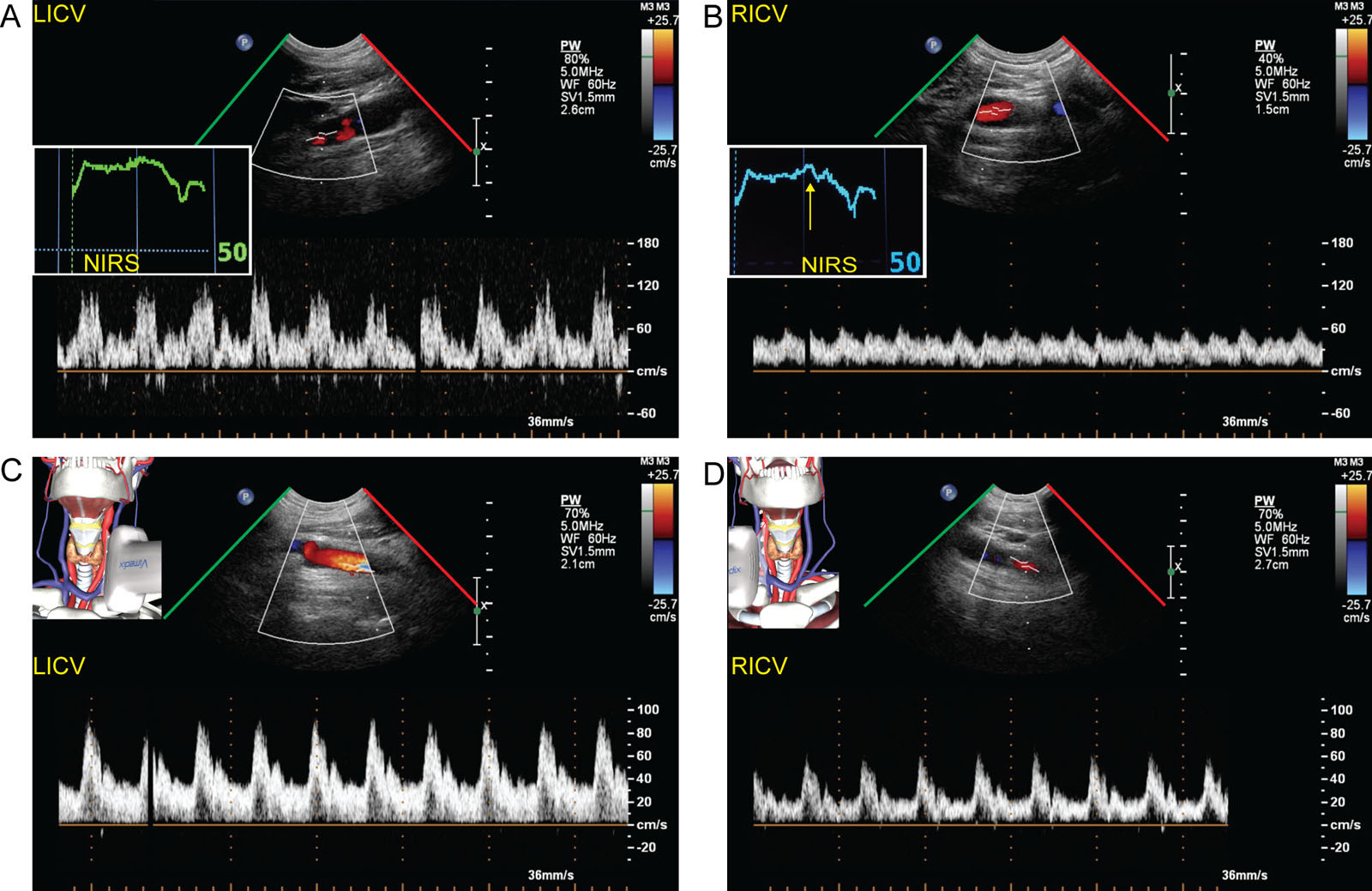
Carotid perfusion in aortic dissection. Surface ultrasound of the (A) left and (B) right carotid artery during clamping of the right innominate artery shows reduced RICV but minimal reduction in the right regional brain saturation using NIRS. (C, D) Internal carotid artery signals at the end of the procedure show the right was still lower than the left. Abbreviations: LICV, left internal carotid velocity; NIRS, near-infrared spectroscopy; RICV, right internal carotid velocity.
eFigure 23.39
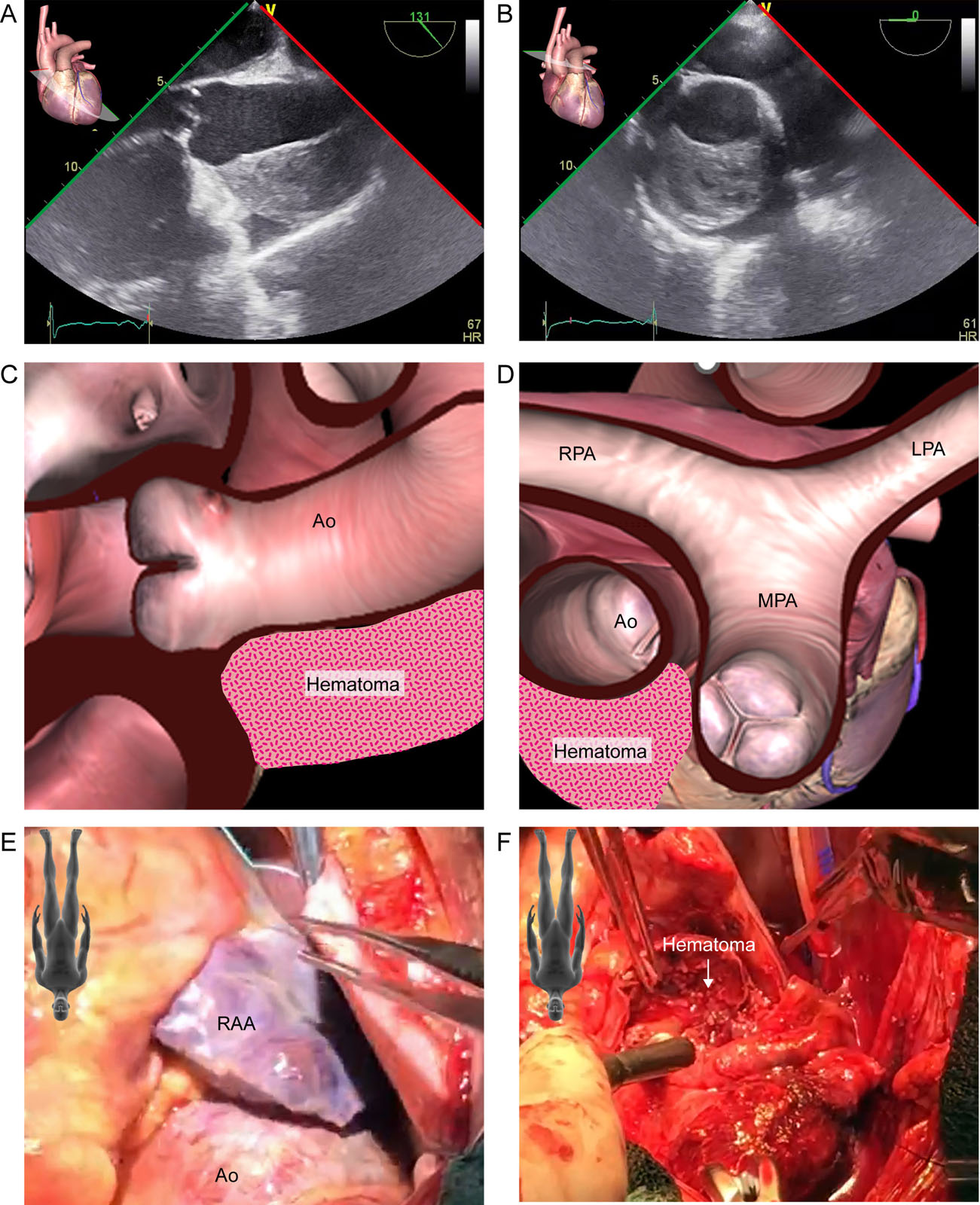
Ascending aorta hematoma. This is a 56-year-old hypertensive man with an acute aortic dissection. (A-D) ME AoV LAX and Asc Ao SAX views show an aortic hematoma in the anterior wall. (E, F) These are intraoperative photos of the (E) enlarged aorta and (F) mural hematoma. Abbreviations: Ao, aorta; AoV, aortic valve; Asc Ao, ascending aorta; LAX, long-axis; LPA, left pulmonary artery; ME, mid-esophageal; MPA, main pulmonary artery; RA, right atrium; RAA, right atrial appendage; RPA, right pulmonary artery; SAX, short-axis.
Videos
Chapter 23 Fig03A
Chapter 23 Fig03C
Chapter 23 Fig03E
Chapter 23 Fig03G
Chapter 23 Fig03I
Chapter 23 Fig03K
Chapter 23 Fig03M
Chapter 23 Fig05A
Chapter 23 Fig06ABDEGH
Chapter 23 Fig10A2
Chapter 23 Fig10ADG
Chapter 23 Fig10B
Chapter 23 Fig10D
Chapter 23 Fig10EH
Chapter 23 Fig10G
Chapter 23 Fig10J1J2
Chapter 23 Fig10K
Chapter 23 Fig11A
Chapter 23 Fig11D
Chapter 23 Fig11G
Chapter 23 Fig11I
Chapter 23 Fig12A
Chapter 23 Fig13A
Chapter 23 Fig13B
Chapter 23 Fig13DE
Chapter 23 Fig13GH
Chapter 23 Fig13J
Chapter 23 Fig13K
Chapter 23 Fig13M
Chapter 23 Fig13N
Chapter 23 Fig14A
Chapter 23 Fig14C
Chapter 23 Fig14D
Chapter 23 Fig18A
Chapter 23 Fig18B
Chapter 23 Fig18D
Chapter 23 Fig19A
Chapter 23 Fig19B
Chapter 23 Fig20A
Chapter 23 Fig21C
Chapter 23 Fig21D
Chapter 23 Fig21F
Chapter 23 fig22A
Chapter 23 Fig22D
Chapter 23 Fig22F
Chapter 23 Fig24GI
Chapter 23 Fig25A
Chapter 23 Fig25E
Chapter 23 Fig25G
Chapter 23 Fig26A
Chapter 23 Fig26B
Chapter 23 Fig26D
Chapter 23 Fig27A
Chapter 23 Fig27C
Chapter 23 Fig28A
Chapter 23 Fig28C
Chapter 23 Fig29A
Chapter 23 Fig29B
Chapter 23 Fig29C
Chapter 23 Fig30A
Chapter 23 Fig32A
Chapter 23 Fig32C
Chapter 23 Fig32E
Chapter 23 Fig33A
Chapter 23 Fig33B
Chapter 23 Fig33D
Chapter 23 Fig33E
Chapter 23 Fig33G
Chapter 23 Fig33H
Chapter 23 Fig35A
Chapter 23 Fig36C
Chapter 23 Fig38A
Chapter 23 Fig38F
Chapter 23 Fig39A
Chapter 23 Fig39B
Chapter 23 Fig39E
Chapter 23 Fig39F
Chapter 23 Fig40A
Chapter 23 Fig40D
Chapter 23 Fig40G
Chapter 23 Fig41A
Chapter 23 Fig41C
Chapter 23 Fig41D
Chapter 23 Fig42A
Chapter 23 Fig42B
Chapter 23 Fig45A
Chapter 23 Fig45B
Chapter 23 Fig46A
Chapter 23 Fig47A
Chapter 23 Fig47E
Chapter 23 Fig47F
Tables
eTable 23.1 TEE views for assessing the aorta
TEE View |
View-Technique |
Utility/Disadvantages |
 |
ME Ascending aorta LAX |
|
 |
ME Ascending aorta SAX |
|
 |
Descending aorta SAX |
|
 |
Descending aorta LAX Angle: 90-100° |
|
 |
UE Aortic arch LAX |
|
 |
UE Aortic arch SAX |
|
 |
UE LSCA |
|
 |
UE LCCA |
|
 |
UE RBCA |
|
 |
DTG Aortic arch |
|
Abbreviations: AoV, aortic valve; AR, aortic regurgitation; CWD, continuous wave Doppler; DTG, deep transgastric; LAX, long-axis; LCCA, left common carotid artery; LSCA, left subclavian artery; LVOT, left ventricular outflow tract; ME, mid-esophageal; PDA, patent ductus arteriosus; PV, pulmonic valve; PWD, pulsed wave Doppler; RBCA, right brachiocephalic artery; SAX, short-axis; TEE, transesophageal echocardiography; UE, upper esophageal. Adapted from Hahn et al.66 |
||