Figures
eFigure 24.4
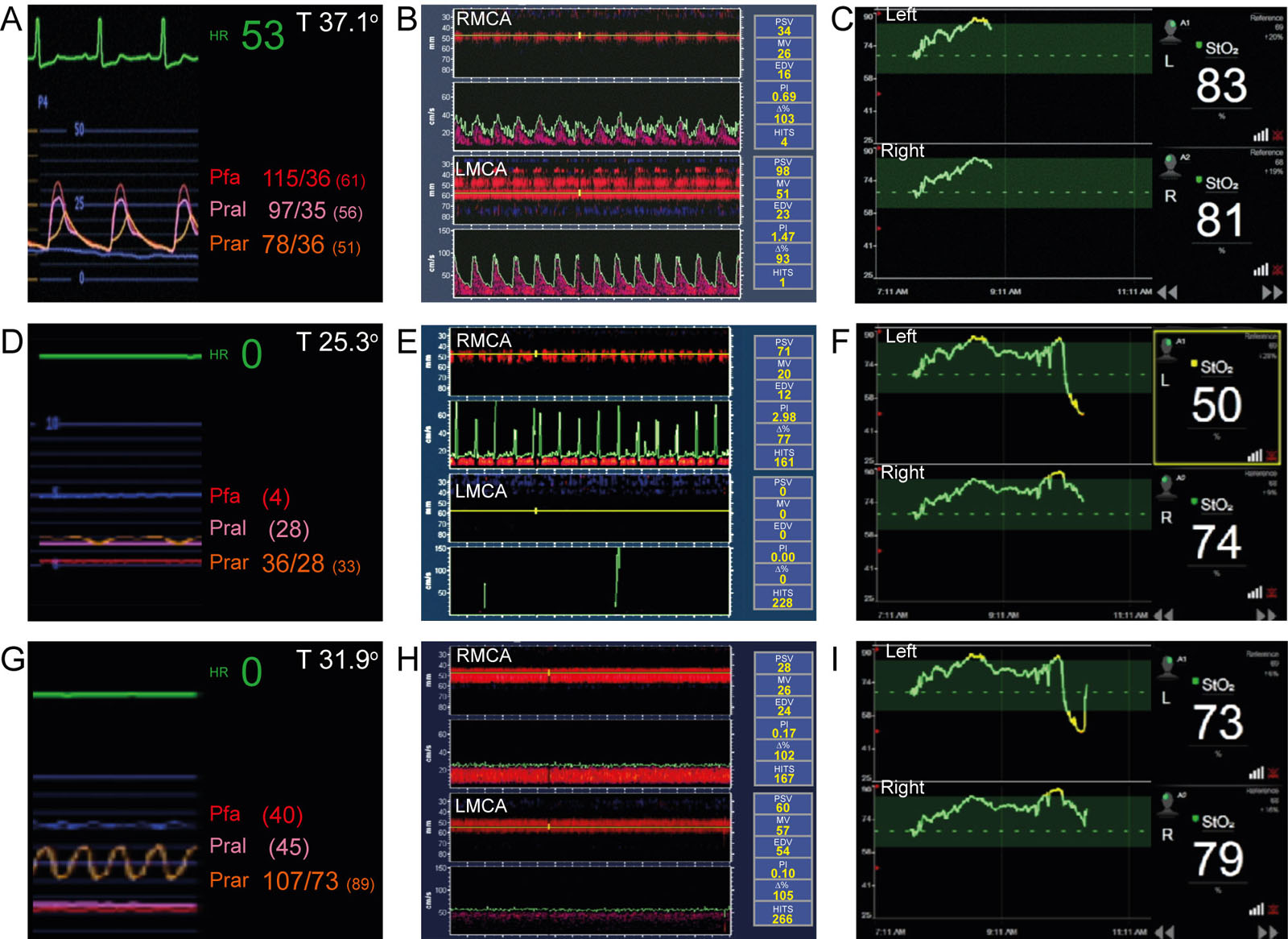
Antegrade perfusion and circulatory arrest. This is a 62-year-old man with aortic dissection type A and AxA cannulation with antegrade cerebral perfusion. (A-C) These are the baseline pressure, TCD and NIRS values. (D-F) Upon initiation of circulatory arrest, there was a reduction in the LMCA velocities causing brain desaturation. (G-I) Central aortic cannulation reestablished normal bilateral reperfusion and brain saturation. Abbreviations: %, percentage of mean velocity in relation to the baseline value; AxA, axillary artery; EDV, end-diastolic velocity; HITS, high-intensity transient signals;HR, heart rate; LMCA, left middle cerebral artery; MV, mean velocity; NIRS, near-infrared spectroscopy; Pfa, femoral arterial pressure; PI, pulsatility index; Pral, left radial artery pressure; Prar, right radial artery pressure; PSV, peak systolic velocity; RMCA, right middle cerebral artery; StO2, tissue oxygen saturation; T, temperature; TCD, transcranial Doppler.
eFigure 24.9
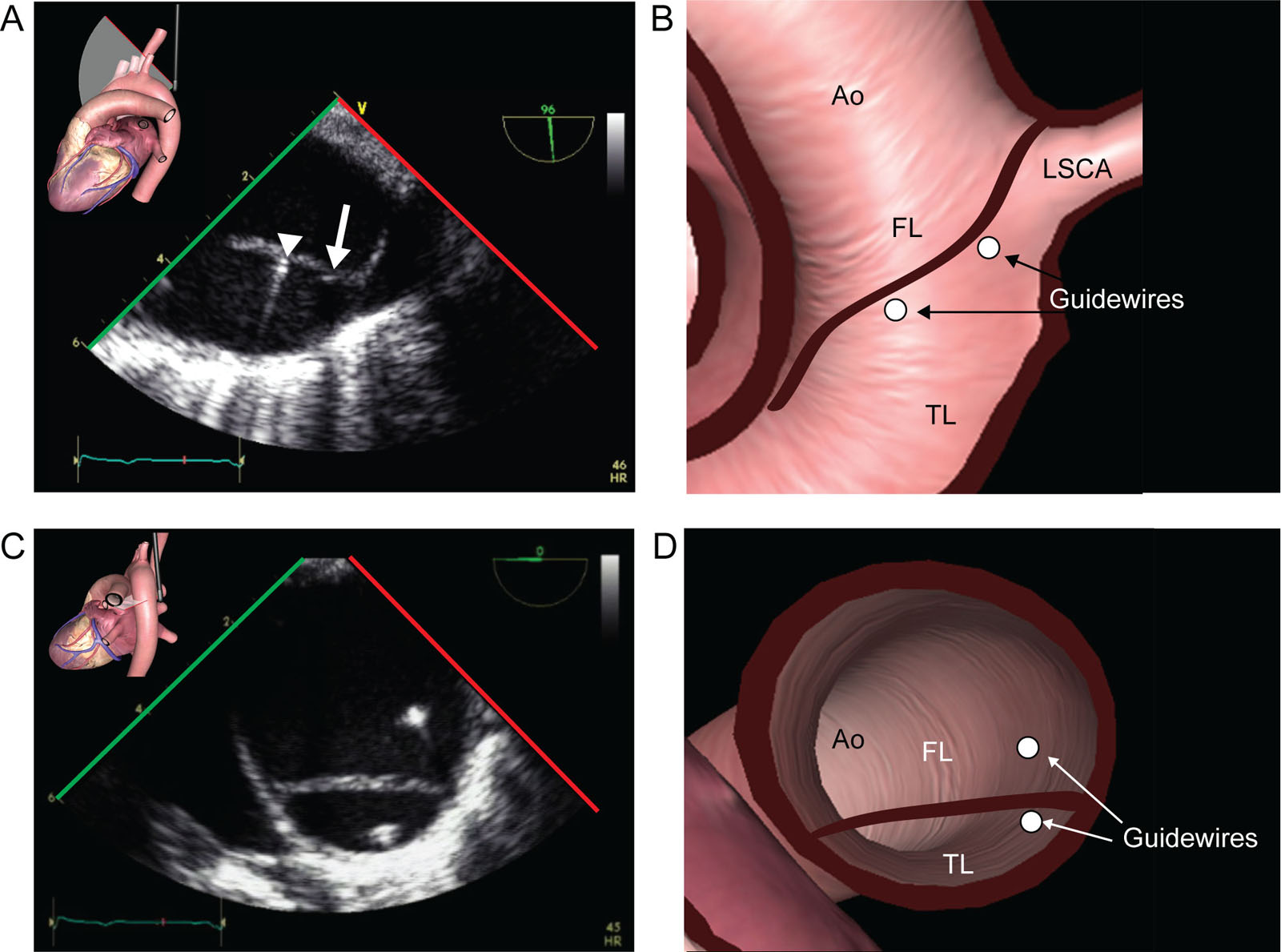
Guidewire position in aortic dissection. (A,B) UE aortic arch LAX view at 90° near the LSCA level shows a type B aortic dissection during TEVAR. The angiography catheter (arrowhead) and the stent-graft delivery catheter wire (small arrow) both appear during retrograde advancement in the TL. (C,D) Descending Ao SAX view in a patient with an aortic dissection shows different guidewires, one correctly in the TL and one incorrectly in the FL. Abbreviations: Ao, aorta; FL, false lumen; LAX, long-axis; LSCA, left subclavian artery; SAX, short-axis; TEVAR, thoracic endovascular aortic repair; TL, true lumen; UE, upper esophageal.
eFigure 24.10
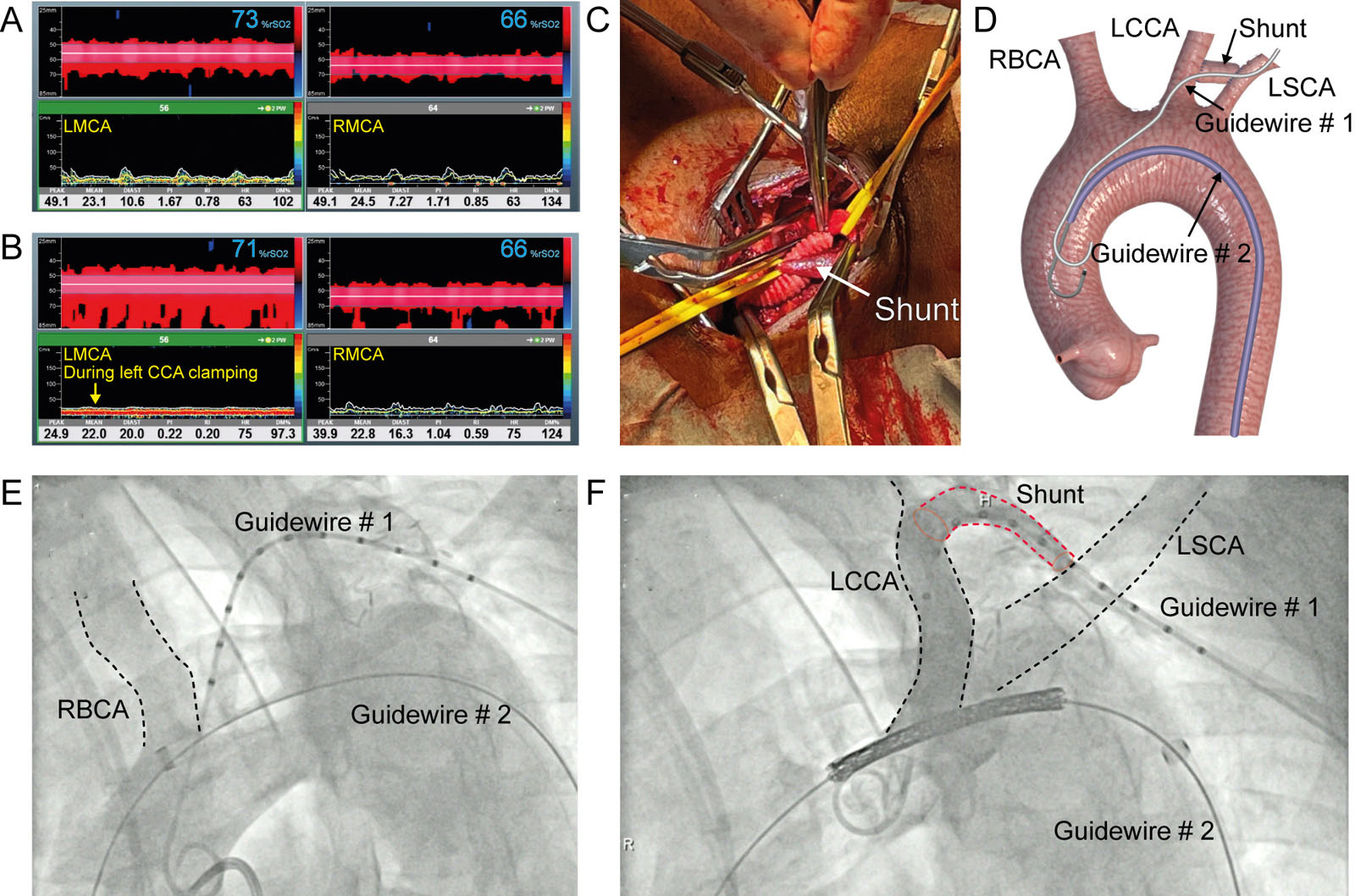
Aortic coarctation in a 45-year-old man who underwent a LCCA to LSCA shunt prior to aortic arch stent insertion. (A-D) TCD of the LMCA and RMCA TCD and intraoperative field (E) before and (F) during carotid clamping. Note in (B) the loss of the pulsatility on the left TCD signal (arrow) with only a small reduction in regional brain saturation (rSO2) from 73% to 71% on the left side. Abbreviations: Diast, diastole; DM%: percent difference in the mean velocity compared to baseline; HR, heart rate; LCCA, left common carotid artery; LMCA, left middle cerebral artery; LSCA, left subclavian artery; PI, pulsatility index; RI, resistance index; RBCA, right brachiocephalic artery; RMCA, right middle cerebral artery; rSO2, regional brain saturation; TCD, transcranial Doppler (Courtesy of Dr. Marina Ibrahim)
Videos
Chapter 24 Fig02G
Chapter 24 Fig03B
Chapter 24 Fig04
Chapter 24 Fig05A
Chapter 24 Fig07A
Chapter 24 Fig07C
Chapter 24 fig07F
Chapter 24 Fig07G
Chapter 24 Fig09A
Chapter 24 Fig09C
Chapter 24 Fig10A
Chapter 24 Fig10B
Chapter 24 Fig10C
Chapter 24 Fig11A
Chapter 24 Fig11C
Chapter 24 Fig12A
Chapter 24 Fig12C
Chapter 24 Fig14A
Chapter 24 Fig14C
Chapter 24 Fig14D
Chapter 24 Fig15A
Chapter 24 Fig15D
Chapter 24 Fig15FGH
Chapter 24 Fig16A
Chapter 24 Fig16B
Chapter 24 Fig16D
Chapter 24 Fig17A
Chapter 24 Fig17C
Chapter 24 Fig17EF
Chapter 24 Fig20A
Chapter 24 Fig20C
Chapter 24 Fig21A
Chapter 24 Fig22A
Chapter 24 Fig22B
Chapter 24 Fig22D
Chapter 24 Fig22F
Chapter 24 Fig22G
Chapter 24 Fig22H
Chapter 24 Fig23A
Chapter 24 Fig23C
Chapter 24 Fig24A
Tables
eTable 24.2 Criteria for endovascular repair of thoracic aortic disease
|
|
Abbreviations: LSCA, left subclavian artery; Source: Adapted from Lee et al.60 |