Figures
eFigure 25.22
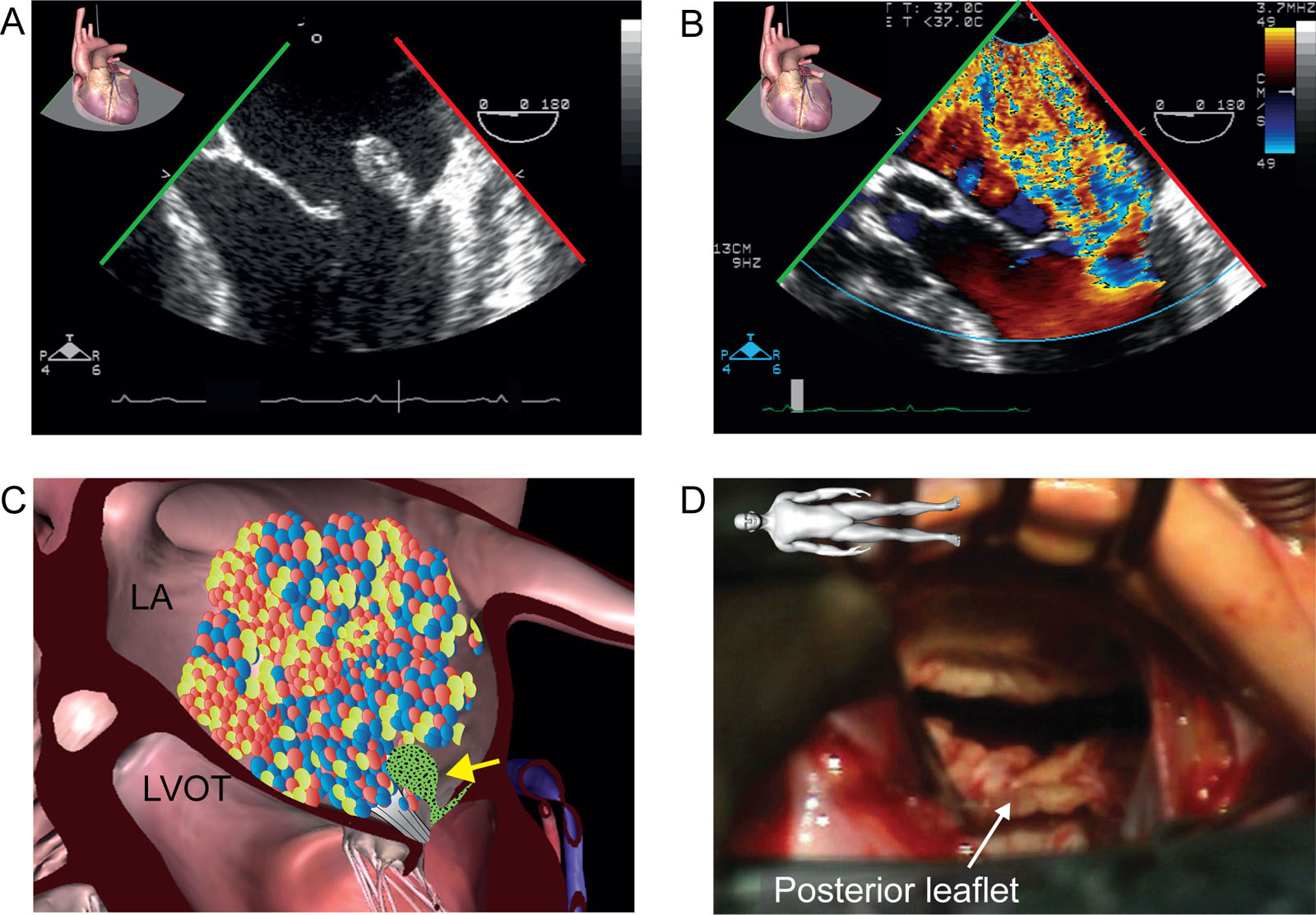
MV endocarditis. This is a 57-year-old man with PMVL endocarditis. (A-D) ME 4C views without and with CFI revealed (A) a vegetation with an associated flail PMVL (P1) scallop and (B) severe MR. (E) Intraoperative photo confirms P1 flail. The patient underwent MV replacement. Abbreviations: 4C, four-chamber; CFI, color flow imaging; LA, left atrium; LVOT, left ventricular outflow tract; ME, mid-esophageal; MR, mitral regurgitation; MV, mitral valve; PMVL, posterior mitral valve leaflet. Photo E courtesy of Dr. Michel Carrier.
eFigure 25.23
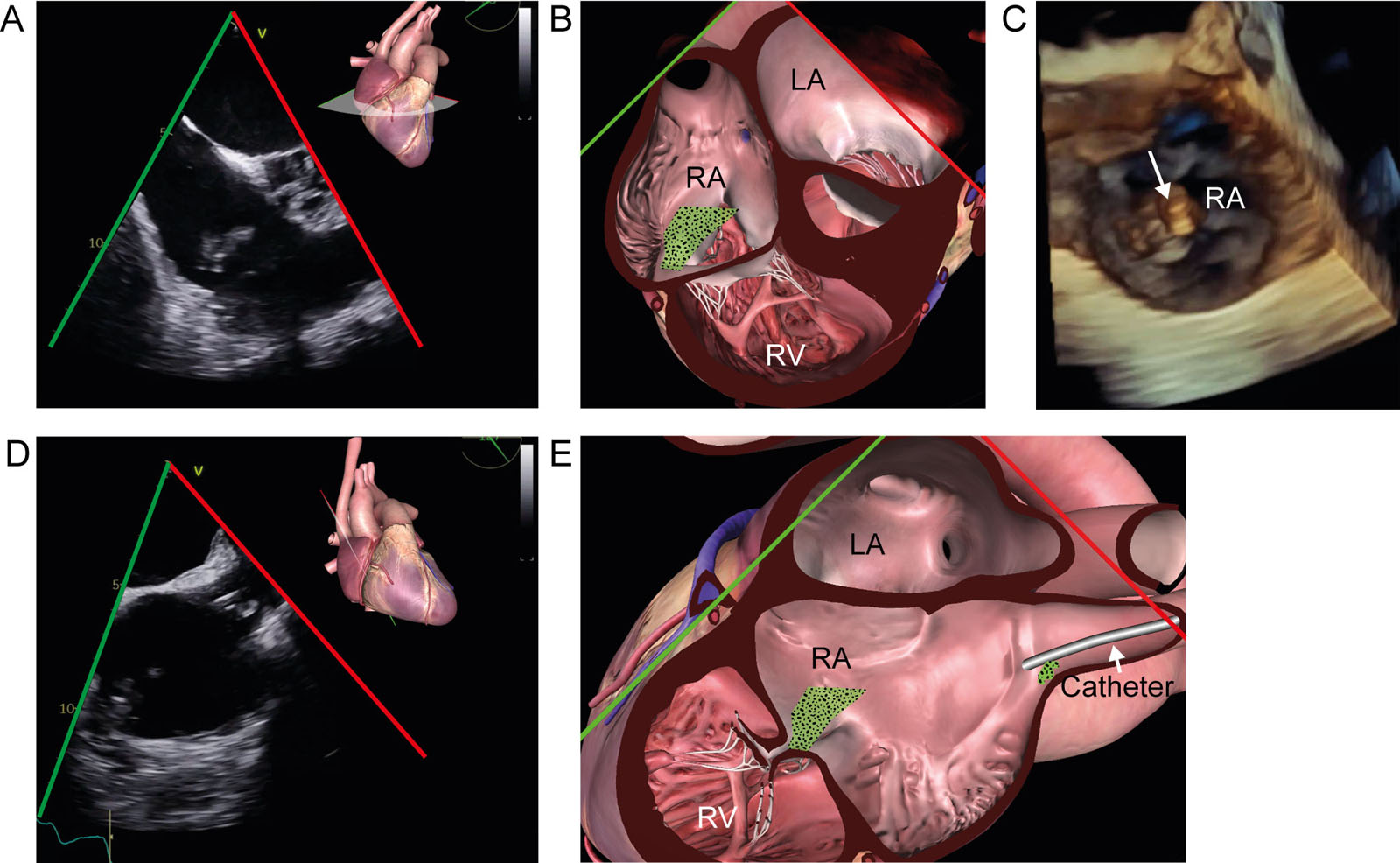
TV endocarditis. (A, B) ME RV-focused view at 35°shows multiple masses attached to the posterior TV leaflet in a bacteremic patient. (C) The 3D dataset from the RA perspective confirms the lesions’ location on the posterior leaflet (arrow). (D, E) The ME 2C RV view also shows a vegetation attached to an SVC catheter. Abbreviations: 2C, two-chamber; 3D, three-dimensional; LA, left atrium; ME, mid-esophageal; RA, right atrium; RV, right ventricle; SVC, superior vena cava; TV, tricuspid valve.
eFigure 25.24
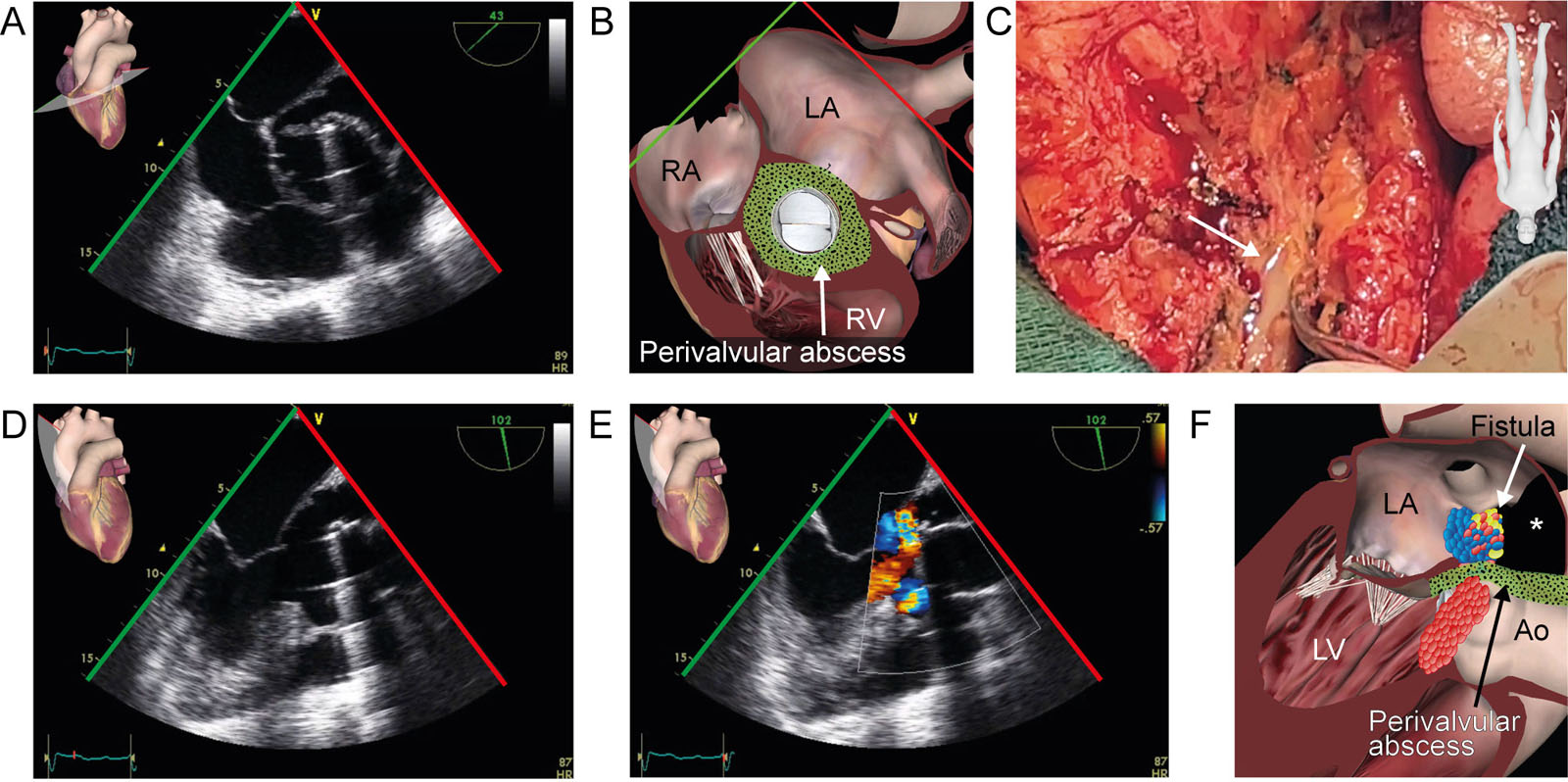
Aortic root pseudoaneurysm. This is a patient post Bentall procedure with composite valve-graft dehiscence. (A, B) ME AoV SAX view at 43° shows a large pseudoaneurysm and a mobile vegetation attached to the aortic composite valve-graft prosthesis. (C) Presence of pericardial effusion. Pus was present upon pericardial opening in this intraoperative photo. (D-F) ME LAX view with CFI shows color directed into the pseudoaneurysm (see *) and through the mechanical composite valve-graft prosthesis in systole. Abbreviations: Ao, aorta; AoV, aortic valve; CFI, color flow imaging; LA, left atrium; LAX, long-axis; LV, left ventricle; ME, mid-esophageal; RA, right atrium; RV, right ventricle; SAX, short-axis.
eFigure 25.25
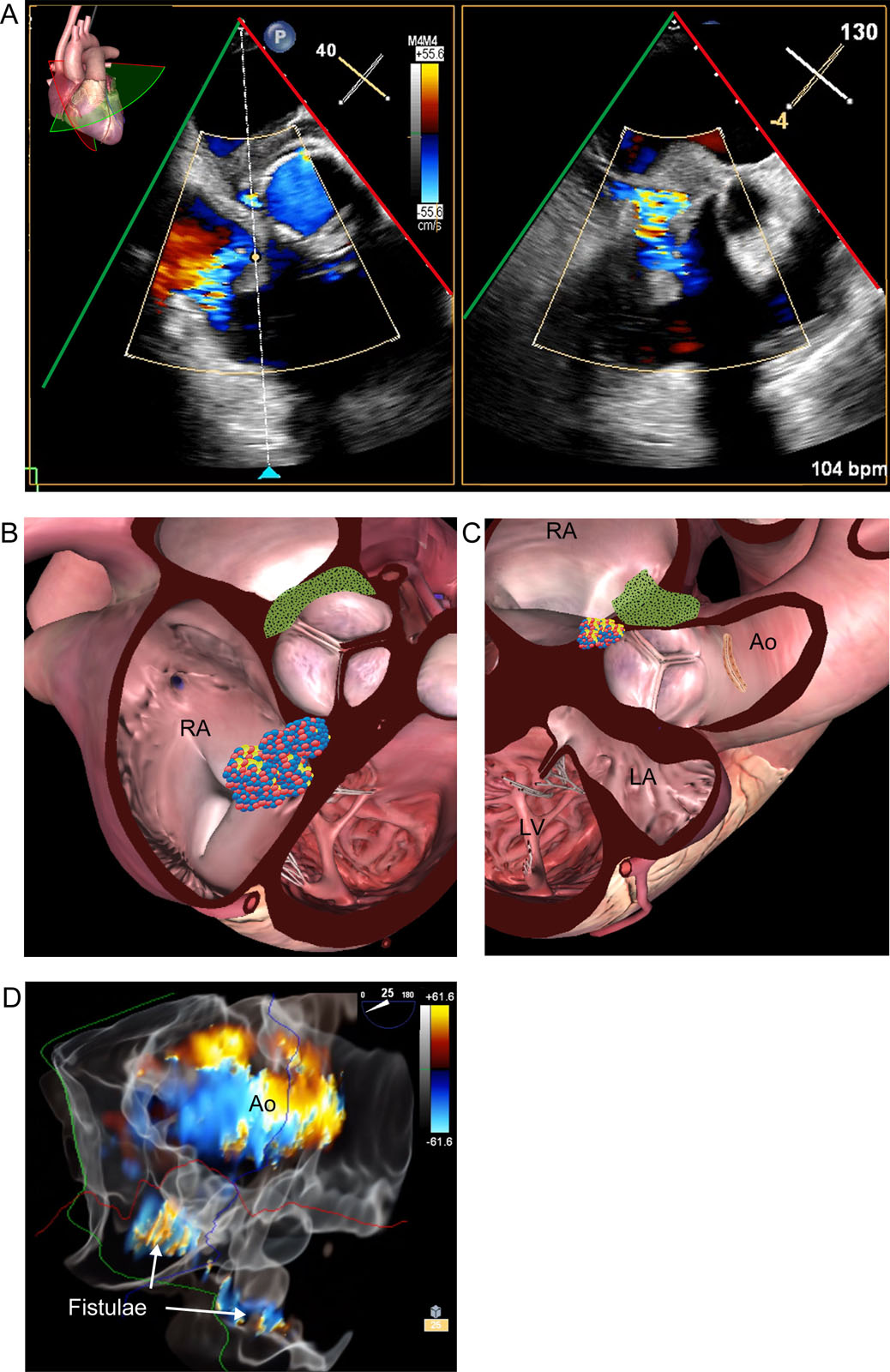
Endocarditis fistula. This is a 65-year-old man with a previous Yacoub procedure. (A-B) Biplane ME RV inflow-outflow view with CFI in diastole shows turbulent flow from the aorta to RA consistent with an aorto-RA fistula. (C) 3D glass view with CFI of the AoV in SAX from the aortic perspective shows the fistula adjacent to the AoV. Abbreviations: 3D, three-dimensional; Ao, aorta; AoV, aortic valve; CFI, color flow imaging; LA, left atrium; LV, left ventricle; ME, mid-esophageal; RA, right atrium; RV, right ventricle; SAX, short-axis.
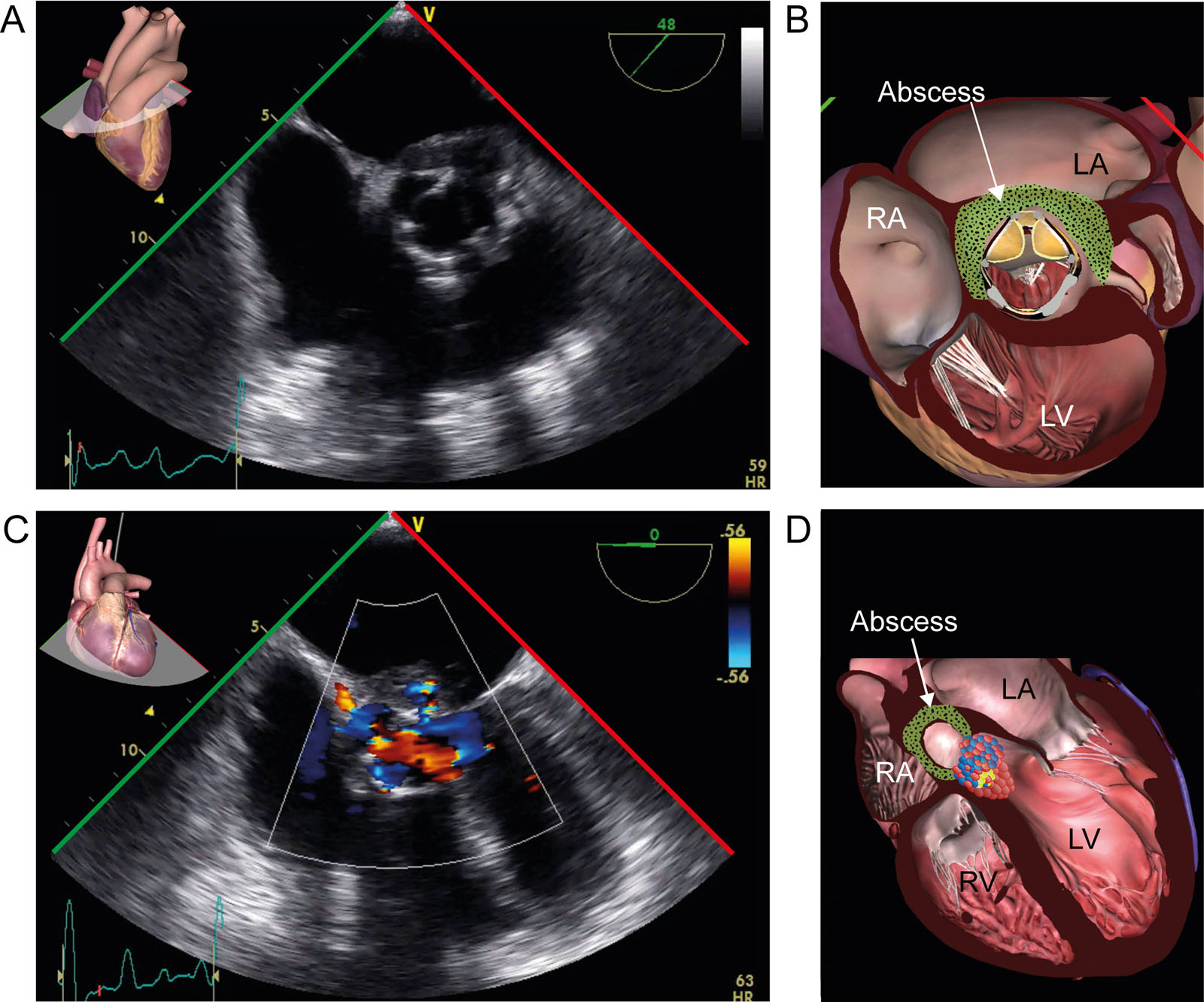
eFigure 25.26
Prosthetic AoV abscess. (A, B) ME AoV SAX view demonstrates a heterogenous mass with echolucent areas at the aorto-mitral curtain level, suggesting a bioprosthetic AoV abscess. (C,D) On CFI, there is no fistula. Abbreviations: AoV, aortic valve; CFI, color flow imaging; LA, left atrium; LV, left ventricle; ME, mid-esophageal; RA, right atrium; RV, right ventricle; SAX, short-axis.
Videos
Chapter 25 Fig02A
Chapter 25 Fig03A
Chapter 25 Fig03B
Chapter 25 Fig03D
Chapter 25 Fig03E
Chapter 25 Fig04A
Chapter 25 Fig04C
Chapter 25 Fig04D
Chapter 25 Fig05A
Chapter 25 Fig05C
Chapter 25 Fig05D
Chapter 25 Fig06A
Chapter 25 Fig06C
Chapter 25 Fig07A
Chapter 25 Fig08A
Chapter 25 Fig08C
Chapter 25 Fig09A
Chapter 25 Fig09C
Chapter 25 Fig09E
Chapter 25 Fig10A
Chapter 25 Fig10C
Chapter 25 Fig11A
Chapter 25 Fig11C
Chapter 25 Fig11D
Chapter 25 Fig12AC
Chapter 25 Fig12D
Chapter 25 Fig12E
Chapter 25 Fig12F
Chapter 25 Fig13A
Chapter 25 Fig13C
Chapter 25 Fig13D
Chapter 25 Fig13F
Chapter 25 Fig14A
Chapter 25 Fig14C
Chapter 25 Fig15A
Chapter 25 Fig15B
Chapter 25 Fig15E
Chapter 25 Fig17C
Chapter 25 Fig18C
Chapter 25 Fig18E
Chapter 25 Fig18F
Chapter 25 Fig18H
Chapter 25 Fig19A
Chapter 25 Fig20A
Chapter 25 Fig20C
Chapter 25 Fig20E
Chapter 25 Fig21A
Chapter 25 Fig21C
Chapter 25 Fig22A
Chapter 25 Fig22B
Chapter 25 Fig22D
Chapter 25 Fig23A
Chapter 25 Fig23C
Chapter 25 Fig23D
Chapter 25 Fig24A
Chapter 25 Fig24C
Chapter 25 Fig24D
Chapter 25 Fig24E
Chapter 25 Fig25A
Chapter 25 Fig25D
Chapter 25 Fig26A
Chapter 25 Fig26C
Chapter 25 Fig27A
Chapter 25 Fig27CDE
Chapter 25 Fig28A
Chapter 25 Fig28C
Chapter 25 Fig28D
Chapter 25 Fig28F
Tables
eTable 25.2 Clinica and imaging features to distinguish benign and malignant cardiac masses
| Feature | Favors benign cardiac mass | Favors malignant cardiac mass |
| Size and rate of growth | Smaller size; slow growing (1-4 mm/month) | Usually larger size; faster growing (5-15 mm/month) |
| Location | Left atrial location | Non-left side location |
| Systemic features | Usually absent (except fever in 14% of myxomas) | Weight loss; constitutional symptoms and symptoms of primary malignancy |
| Pericardial involvement | Unusual | Pericardial effusion commonly seen, usually hemorrhagic; pericardial invasion and/or seeding may be present (nodular studding) |
| Myocardial infiltration | Usually none (except fibromas, rhabdomyomas or lipomas, arising in the myocardium) | Direct invasion of myocardial tissue originating from outside heart or a cardiac chamber cavity often seen |
| Coronary artery involvement | No involvement, although extrinsic compress can occur with large benign masses (fibrotic encasement of the coronary arteries may occur in Erdheim-Chester disease) | Coronary arterial encasement may appear in lymphoma; other malignant tumors may directly invade coronaries |
| Valvular dysfunction | Usually none (note that fibroelastomas usually involve the valve leaflets and, if large, may cause regurgitation) | Direct invasion of valve apparatus or annulus is not common but possible |
| Arrhythmia | Less common with benign masses unless large size or specific location | Atrioventricular block, bundle branch block, conduction abnormalities, and ventricular arrhythmias are more common with myocardial and epicardial invasion by malignant masses |
| Systemic or pulmonary embolism | May occur depending on the chamber or valvular location (e.g., valve papillary fibroelastoma, myxoma) | Commonly seen in metastatic tumors; may also occur from thrombus associated with the malignancy |
| Extra-cardiac masses | Absent (except syndromes such as lentigines, atrial myxomas, and blue nevi and nevi, atrial myxoma, myxoid neurofibromas, and ephelides may have extracardiac myxomas, neurofibromas, and other tumors) | Usually present (site of primary malignancy, or other metastatic sites) |
| Obstruction | Valvular or outflow tract obstruction can rarely occur with large mural benign tumors, e.g., myxomas | Superior vena cava obstruction is more common with right-sided malignant lesions (e.g., angiosarcoma, metastatic lung, breast cancer, lymphoma, thymoma, and germ cell tumors) |
| LGE on CMR | No LGE (except fibromas and most myxomas) | LGE is almost always present. |
| First-pass perfusion on CMR (gadolinium) or echocardiography (ultrasound-enhancing agent) | Most do not show high vascularity (except for hemangiomas ‘‘sunray’’ appearance). | Strong contrast uptake (ie high vascularity) |
| Abbreviations: CMR, cardiac magnetic resonance; LGE, late gadolinium enhancement. Adapted from Rout et al.53 | ||
eTable 25.3 2023 Duke-International Society for Cardiovascular Infectious Diseases IE Criteria
| Major criteria | Minor criteria |
| Microbiological major criteria | Predisposition fFever greater than 38.0 °C Vascular phenomena g Immunologic phenomena hMicrobiologic evidence, falling short of a major criterionImaging criteria abnormal iPhysical examination criteria j |
| Positive blood culture aPositive laboratory test b | |
| Imaging major criteria | |
| Echocardiography and CT imaging cPET CT with [18F] FDG imaging dSurgical major criteria e | |
| Definite endocarditis = 2 major criteria or 1 major + 3 minor or 5 minor Possible endocarditis = 1 major + 1 minor or 3 minor | |
| a Microorganisms that commonly cause (Typical) IE isolated from 2 or more separate blood culture sets or those that occasionally or rarely cause IE isolated from 3 or more separate blood culture sets (Nontypical) b Positive PCR testing c Including vegetation, valvular/leaflet perforation, valvular/leaflet aneurysm, abscess, pseudoaneurysm, intracardiac fistula, significant new valvular regurgitation on echocardiography as compared with previous imaging (Worsening or changing of preexisting regurgitation is not sufficient), or new partial dehiscence of prosthetic valve as compared with previous imaging d Abnormal metabolic activity involving a native or prosthetic valve, ascending aortic graft (with concomitant evidence of valve involvement), intracardiac device lead, or other prosthetic material. e Evidence of IE documented by direct inspection during heart surgery; absence of other microbiologic, imaging, and pathologic criteria f Previous history of IE, prosthetic valve, previous valve repair, CHD, more than mild regurgitation or stenosis of any etiology, endovascular CIED, HOCM, injection drug use g Clinical or radiological evidence of arterial emboli, septic pulmonary infarcts, cerebral or splenic abscess, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, Janeway lesions, purulent purpura h Positive rheumatoid factor, Osler nodes, Roth spots, or immune complex-mediated glomerulonephritis I Abnormal metabolic activity as detected by [18F] FDG PET/CT within 3 months of implantation of prosthetic valve, ascending aortic graft (with concomitant evidence of valvular involvement), intracardiac device leads or other prosthetic material j New valvular regurgitation identified on auscultation if echocardiography is not available (Worsening or changing of preexisting murmur not sufficient) | |
| Abbreviations: [18F] FDG, 18F-fluorodeoxyglucose; CHD, congenital heart disease; CIED, cardiac implantable electronic device; CCT, cardiac computed tomography; HOCM, hypertrophic obstructive cardiomyopathy; IE, infective endocarditis; PCR, polymerase chain reaction; PET CT, positron emission computed tomography. Adapted from Fowler et al. 54 | |