Figures
eFigure 27.10
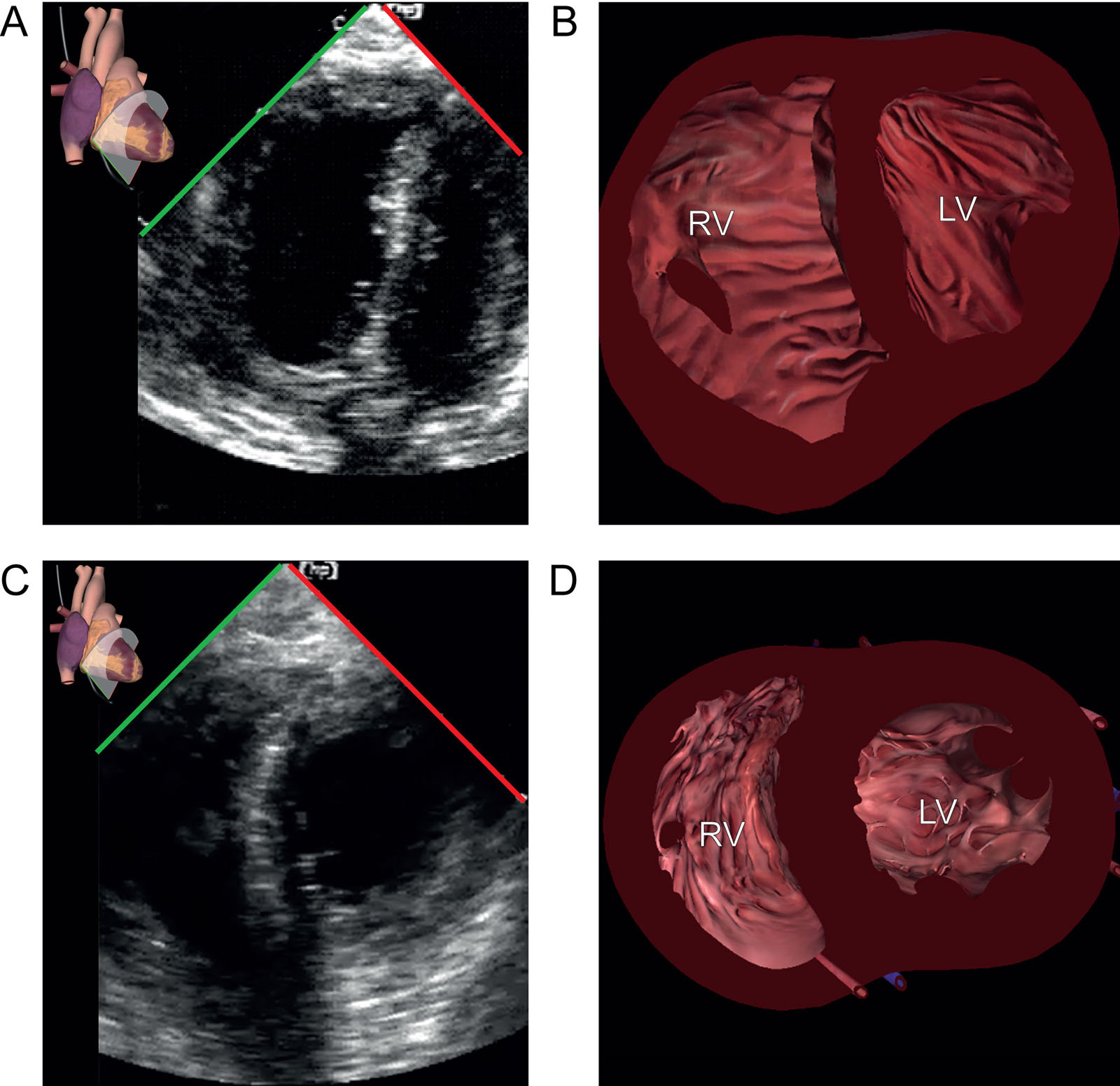
RV dysfunction. This patient undergoing bilateral lung transplantation experiences transient RV dysfunction. (A, B) TG mid SAX view shows significant RV dilatation and a flattened ventricular septum with paradoxical septal motion suggestive of RV failure. This is possibly from PA clamping or air embolization in the RCA. (C, D) The administration of vasoactive support improved RV function. Abbreviations: LV, left ventricle; PA, pulmonary artery; RCA, right coronary artery; RV, right ventricle; SAX, short-axis; TG, transgastric.

eFigure 27.11
Fluid assessment. Preload evaluation during hemodynamic instability after single lung transplantation in a 53-year-old woman with end-stage emphysema. (A, B) Invasive hemodynamic monitoring shows a HR 121 beats/min, Pa 103/62 mmHg, Ppa 29/19 mmHg, Paop 13 mmHg and CVP 14 mmHg (not shown). The capnographic waveform (ETCO2) is typical of a single lung transplant with the initial normal waveform from the transplanted lung, followed by the ascending phase III from obstructive disease (arrow). There is respiratory variation of the saturation signal from the pulse oximeter. (C, D) Despite the relatively normal filling pressures, the LV shows LVESCO suggestive of suboptimal preload in the TG mid-papillary SAX view. The patient’s hemodynamic condition improved with intravenous fluid administration. Abbreviations: ETCO2, end-tidal CO2; HR, heart rate; LV, left ventricle; LVESCO, left ventricular end-systolic cavity obliteration; Pa, arterial pressure; PCWP, pulmonary capillary wedge pressure; Ppa, pulmonary artery pressure; Resp, respiration; SaO2, arterial oxygen saturation; Sat, saturation; SAX, short-axis; TG, transgastric.
eFigure 27.13
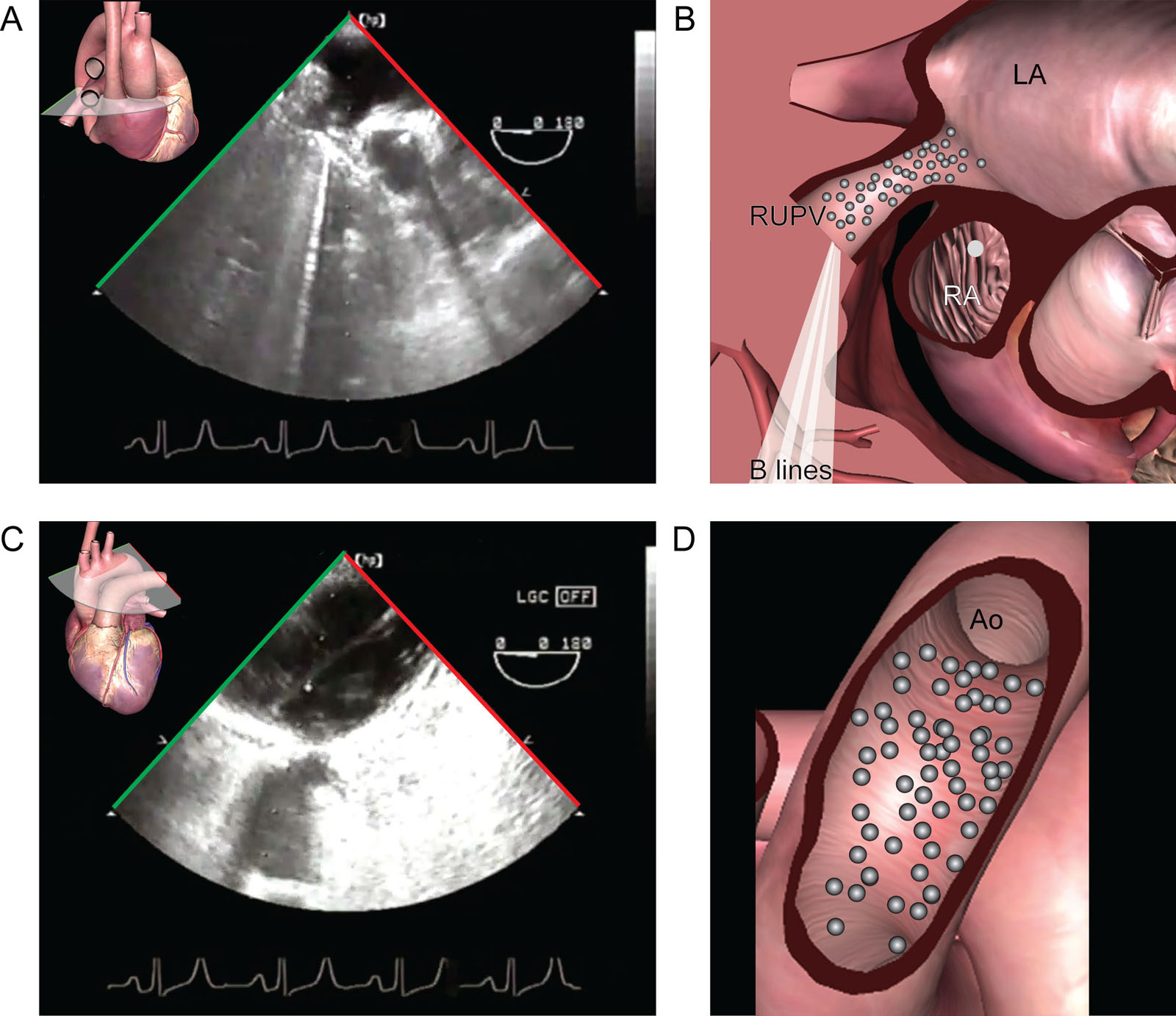
Air emboli in lung transplantation. (A,B) ME view with right-sided rotation shows air bubbles coming the RUPV at the completion of the vascular anastomosis. (C,D) In the UE aortic arch LAX view, there are also air bubbles in the Ao. Abbreviations: Ao, aorta; LA, left atrium; LAX, long-axis; ME, mid-esophageal; RA, right atrium; RUPV, right upper pulmonary vein; UE, upper esophageal.
eFigure 27.14
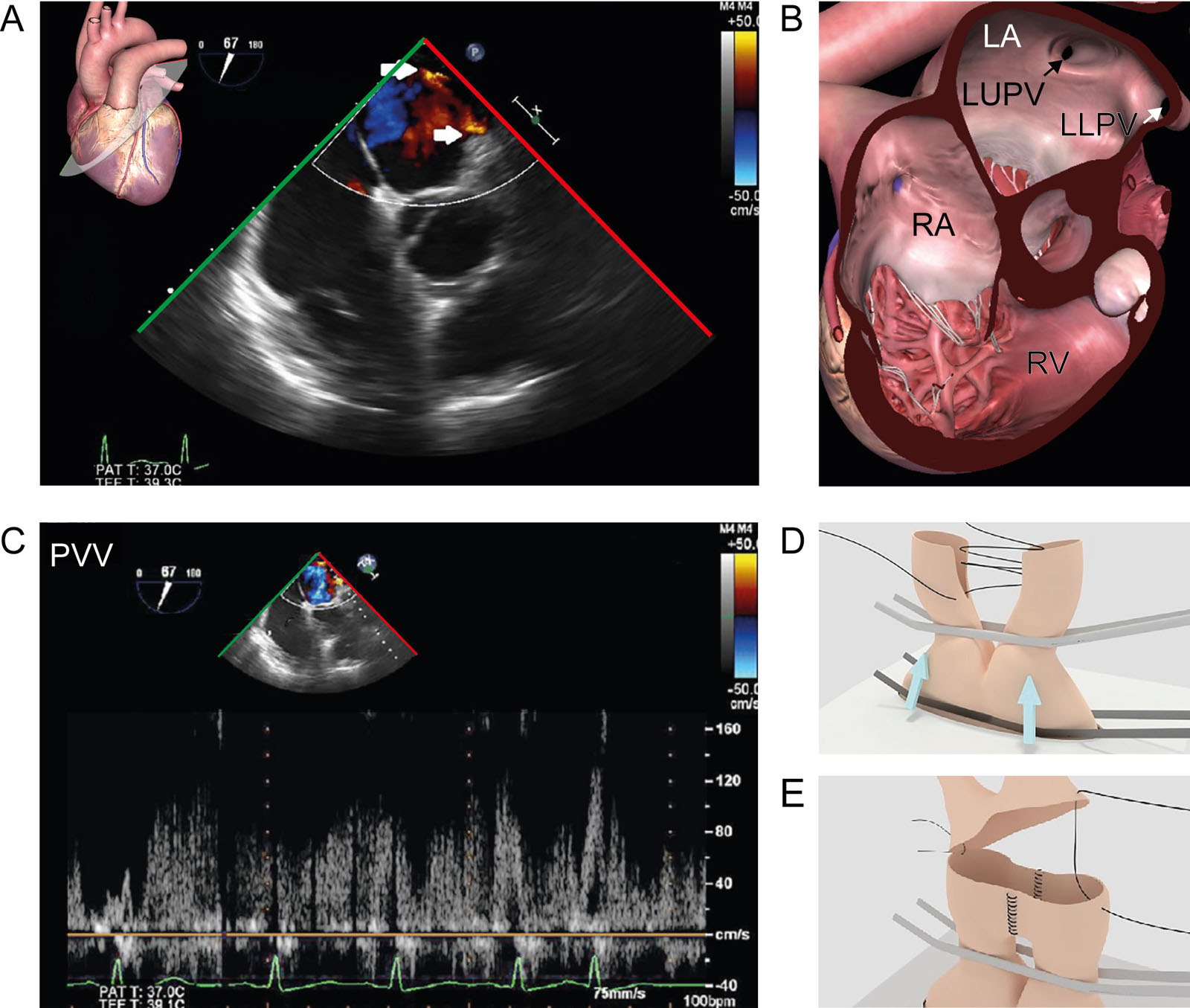
Alternative pulmonary vein anastomosis. (A,B) ME RV inflow-outflow view with CFI shows images post-reperfusion of the left pulmonary vein anastomosis. (C) Pulmonary vein velocity PWD has a full envelope reaching 120 cm/sec. PWD >100 cm/sec indicating turbulent flow. A PV velocity signal with systolic over diastolic wave predominance indicates that PV obstruction causes the high-velocity jets. (D) The Satinsky clamp occludes both pulmonary veins (arrows), thus impeding the construction of the atrial cuff. (E) Cutting a slit in both facing pulmonary veins allowed them to be sewed, forming a common ostium for anastomosis to the atrium. Abbreviations: CFI, color flow imaging; LA, left atrium; LLPV, left lower pulmonary vein; LUPV, left upper pulmonary vein; ME, mid-esophageal; PV, pulmonary vein; PVV, pulmonary venous velocity; PWD, pulsed-wave Doppler; RA, right atrium; RV, right ventricle. Adapted from Luzzi et al.39
eFigure 27.18
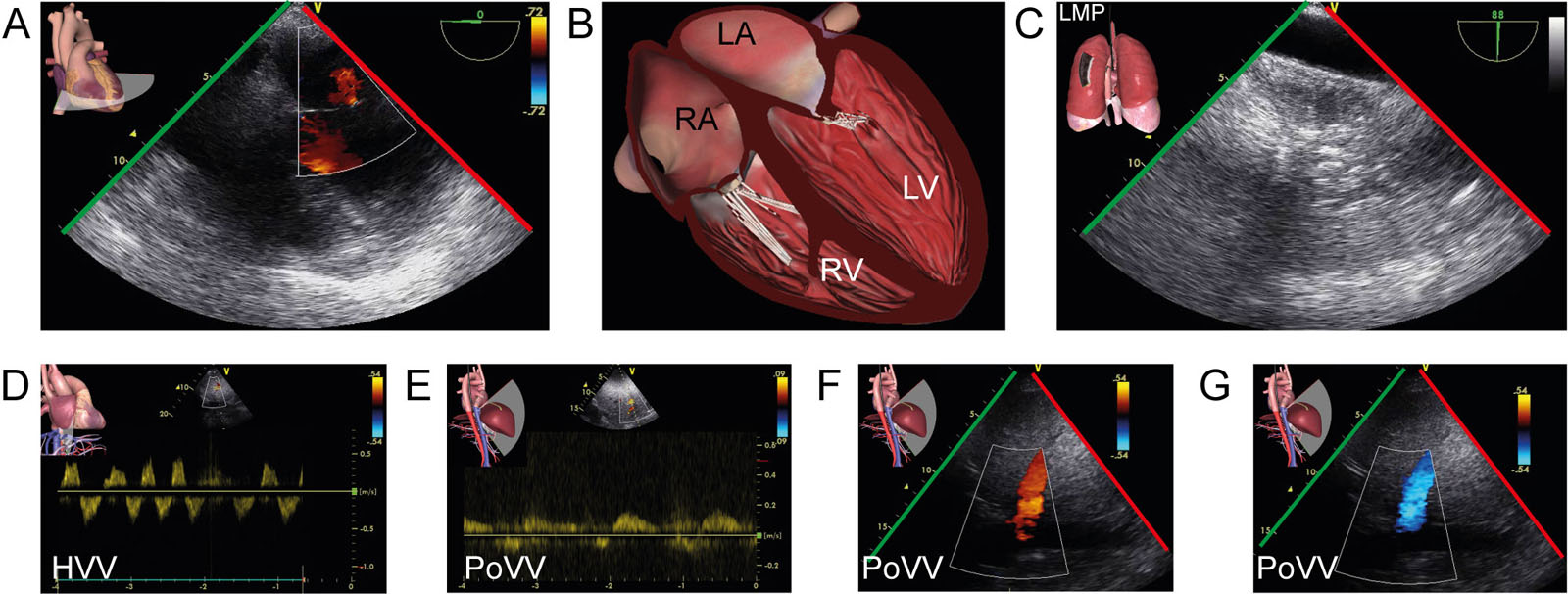
Biventricular failure post lung transplant. (A,B) ME 4C view with CFI in a 56-year-old post-op lung transplant with biventricular septic cardiomyopathy. (C) TELUS of the left lung shows pneumonia that led to a septic shock. (D) TGAUS interrogation of the hepatic vein using PWD revealed a biphasic pattern. (D-F) A similar pattern was present in the portal vein using PWD and CFI with alternating color Doppler signals. Those signals indicate severe RV failure and hepatic venous congestion. Abbreviations: 4C, four-chamber; CFI, color flow imaging; HVV, hepatic vein velocity; LA, left atrium; LMP, left mid posterior; LV, left ventricle; ME, mid-esophageal; PoVV; portal vein velocity; PWD, pulsed-wave Doppler; RA, right atrium; RV, right ventricle; TELUS, transesophageal lung ultrasound; TGAUS, transgastric abdominal ultrasound.
Videos
Chapter 27 Fig01A
Chapter 27 Fig01B
Chapter 27 Fig01CD
Chapter 27 Fig03A
Chapter 27 Fig03B
Chapter 27 Fig03C
Chapter 27 Fig03D
Chapter 27 Fig04A
Chapter 27 Fig04C
Chapter 27 Fig05A
Chapter 27 Fig05C
Chapter 27 Fig05F
Chapter 27 Fig05G
Chapter 27 Fig05H
Chapter 27 Fig06G
Chapter 27 Fig07A
Chapter 27 Fig07B
Chapter 27 Fig07C
Chapter 27 Fig07D
Chapter 27 Fig08A
Chapter 27 Fig08B
Chapter 27 Fig08D
Chapter 27 Fig10AC
Chapter 27 Fig11AB
Chapter 27 Fig11C
Chapter 27 Fig12A
Chapter 27 Fig12C
Chapter 27 Fig13A
Chapter 27 Fig13C
Chapter 27 Fig15A
Chapter 27 Fig15C
Chapter 27 Fig16A
Chapter 27 Fig16CD
Chapter 27 fig17A
Chapter 27 fig17D
Chapter 27 Fig18A
Chapter 27 Fig18C
Chapter 27 Fig19D
Chapter 27 Fig19E
Chapter 27 Fig20A
Chapter 27 Fig20C
Chapter 27 Fig21A
Chapter 27 Fig21B
Chapter 27 Fig22AC
Chapter 27 Fig22F
Tables
eTable 27.1 Indications and contraindications for lung transplantation
Indications |
Consider LungTx for adults with chronic, end-stage lung disease who meet all the following general criteria: |
Absolute Contraindications |
|
|
Relative Contraindications representing factors with high or substantially increased risk |
|
|
Modified from: Consensus document for the selection of lung transplant candidates: An update from the International Society for Heart and Lung Transplantation 2021 1 |
Abbreviations: ACS, acute coronary syndrome; AMR, antibody mediated rejection; BMI, body mass index; CABG, coronary artery bypass grafting; CAD, coronary artery disease; CLAD, chronic lung allograft dysfunction; ECMO, extracorporeal membrane oxygenation; GFR, glomerular filtration rate; HIV, human immunodeficiency virus; LungTx, luung transplantations; LVEF, left ventricular ejection fraction; MI, myocardial infarction; PCI, percutaneous coronary intervention; TB, tuberculosis. |
eTable 27.2 TEE views in lung transplantation
TEE View |
Icon |
View-Technique |
Utility |
 |
ME 4C |
|
|
 |
ME LAX |
|
|
 |
ME Ascending Aorta SAX |
|
|
 |
ME RLPV |
|
|
 |
ME RV Inflow-Outflow |
|
|
 |
ME LUPV |
|
|
 |
ME RUPV |
|
|
 |
ME LPV bifurcation |
|
|
 |
ME RPV bifurcation |
|
|
 |
TG Mid papillary SAX |
|
|
Abbreviations: 4C, four-chamber; Ao, aorta; Asc Ao, ascending aorta; AoV, aortic valve; CFI, color flow imaging; CWD, continuous wave Doppler; IVS, interventricular septum; LA, left atrium; LAX, long-axis; LPV, left pulmonary vein; LUPV, left upper pulmonary vein; LV, left ventricle; LVOTO, left ventricular outflow tract obstruction; ME, mid-esophageal; MV, mitral valve; PA, pulmonary artery; PV, pulmonic valve; PWD, pulsed-wave Doppler; RCA, right coronary artery; RLPV, right lower pulmonary vein; RUPV, right upper pulmonary vein; RPV, right pulmonary vein; RV, right ventricle; RVOTO, right ventricular outflow tract obstruction; SAX, short-axis; SVC, superior vena cava; TEE, transesophageal echocardiography; TG, transgastric; TV, tricuspid valve; Adapted from Hahn et al.36 |
|||