Figures
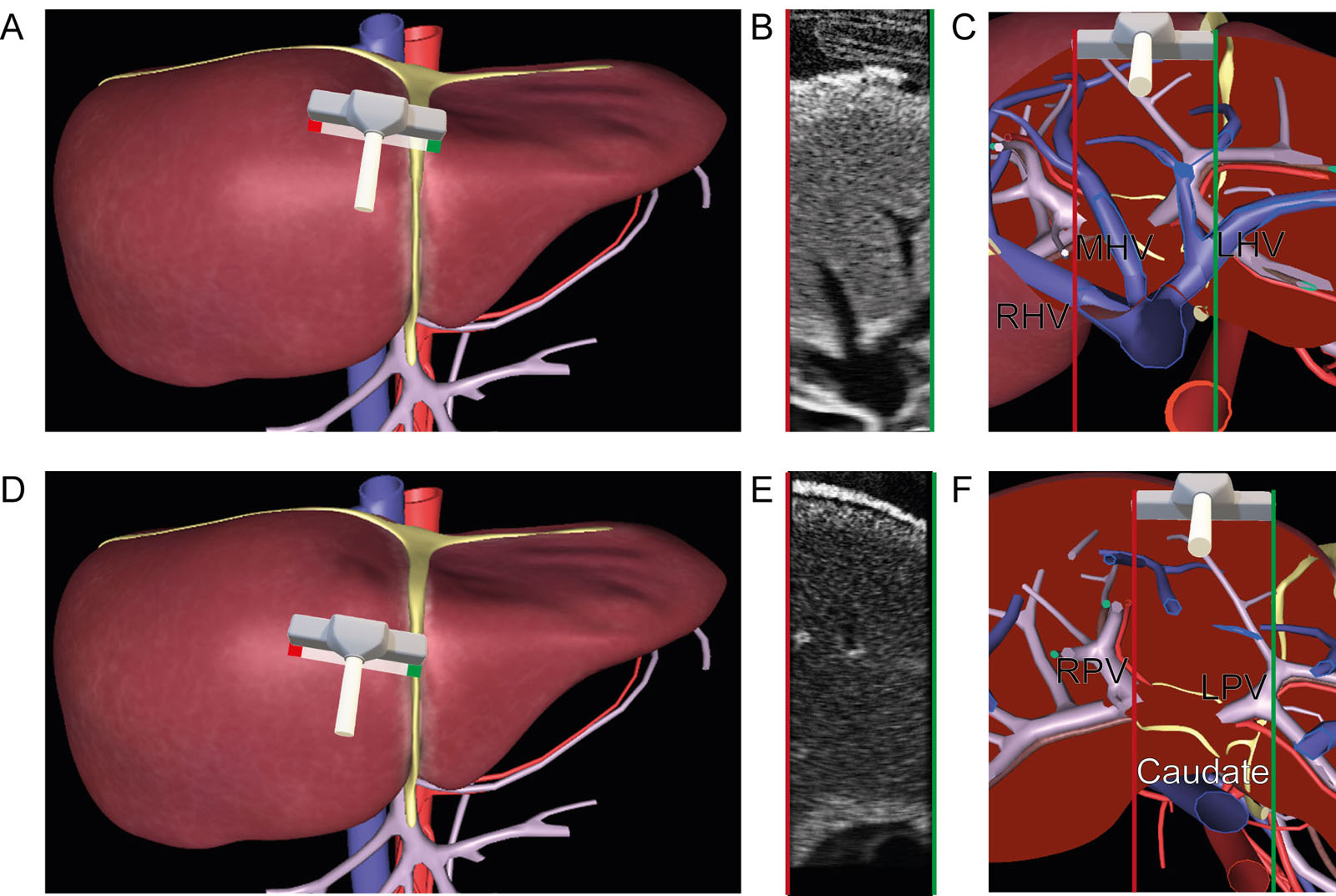
eFigure 28.7
Intraoperative liver surface US scan. These are diagrams of a liver surface US examination of the (A-C) three hepatic veins and the (D-F) caudate lobe (Couinaud segment I) using a linear probe both from a cephalad perspective. The location of the caudate lobe is between the left and right liver lobes, anterior to the IVC, behind the HVs and above the portal vein. It is large in cirrhosis and could narrow the intrahepatic IVC portion. Tilting the probe inferiorly visualizes the portal vein. Abbreviations: HV, hepatic vein; IVC, inferior vena cava; LHV, left hepatic vein; LPV, left portal vein; MHV, middle hepatic vein; RHV, right hepatic vein; RPV, right portal vein; US, ultrasound.
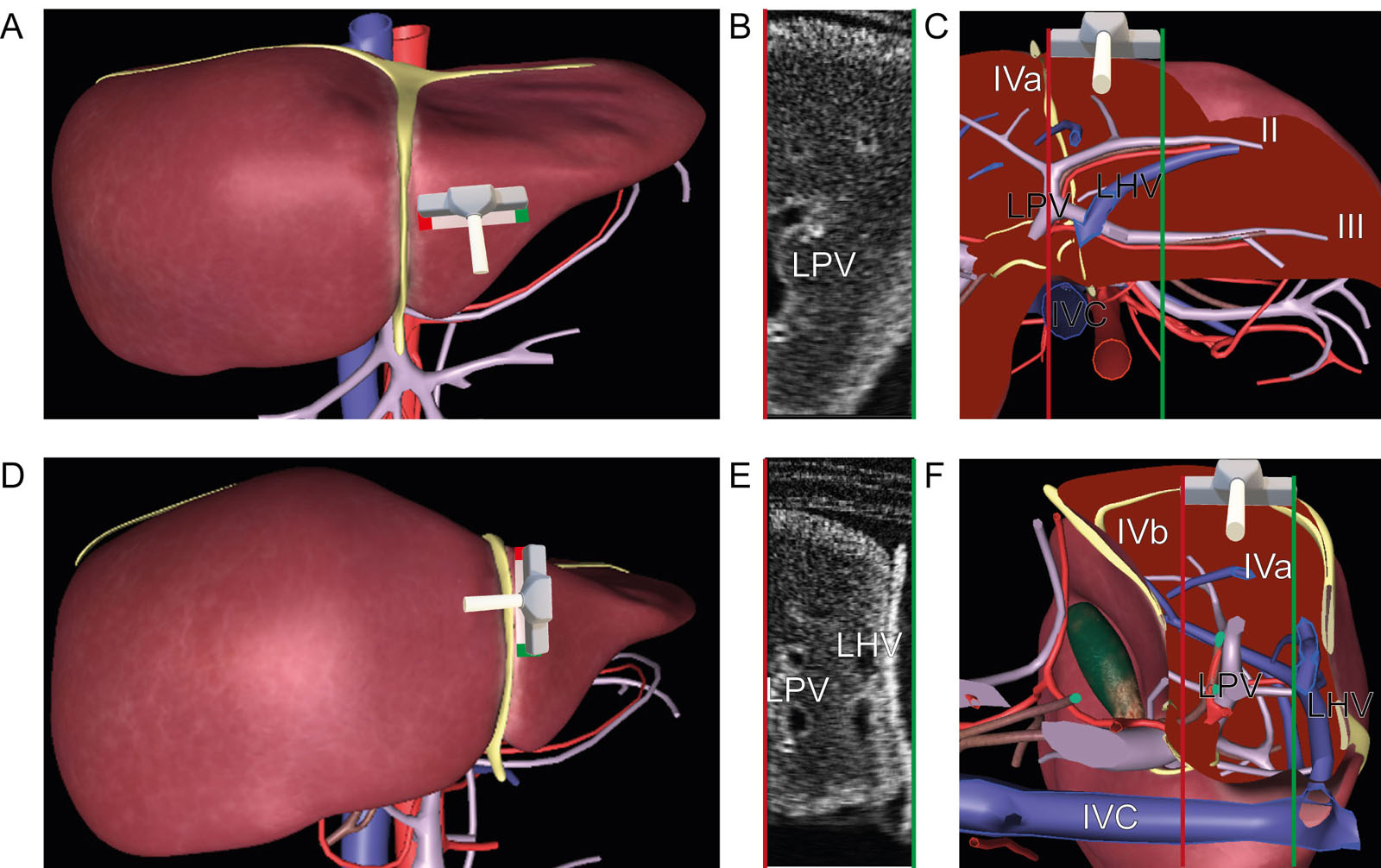
eFigure 28.8
Intraoperative liver surface US scan. These are diagrams of a liver surface US examination with coronal views of the (A-C) LPV and (D-F) RPV and their respective segments from a cephalad perspective. Note the proximity of the hepatic arteries to the portal vessels. Abbreviations: IVC, inferior vena cava; LPV, left portal vein; RPV, right portal vein; US, ultrasound. (See Figure 28.2 for Couinaud segments identification)
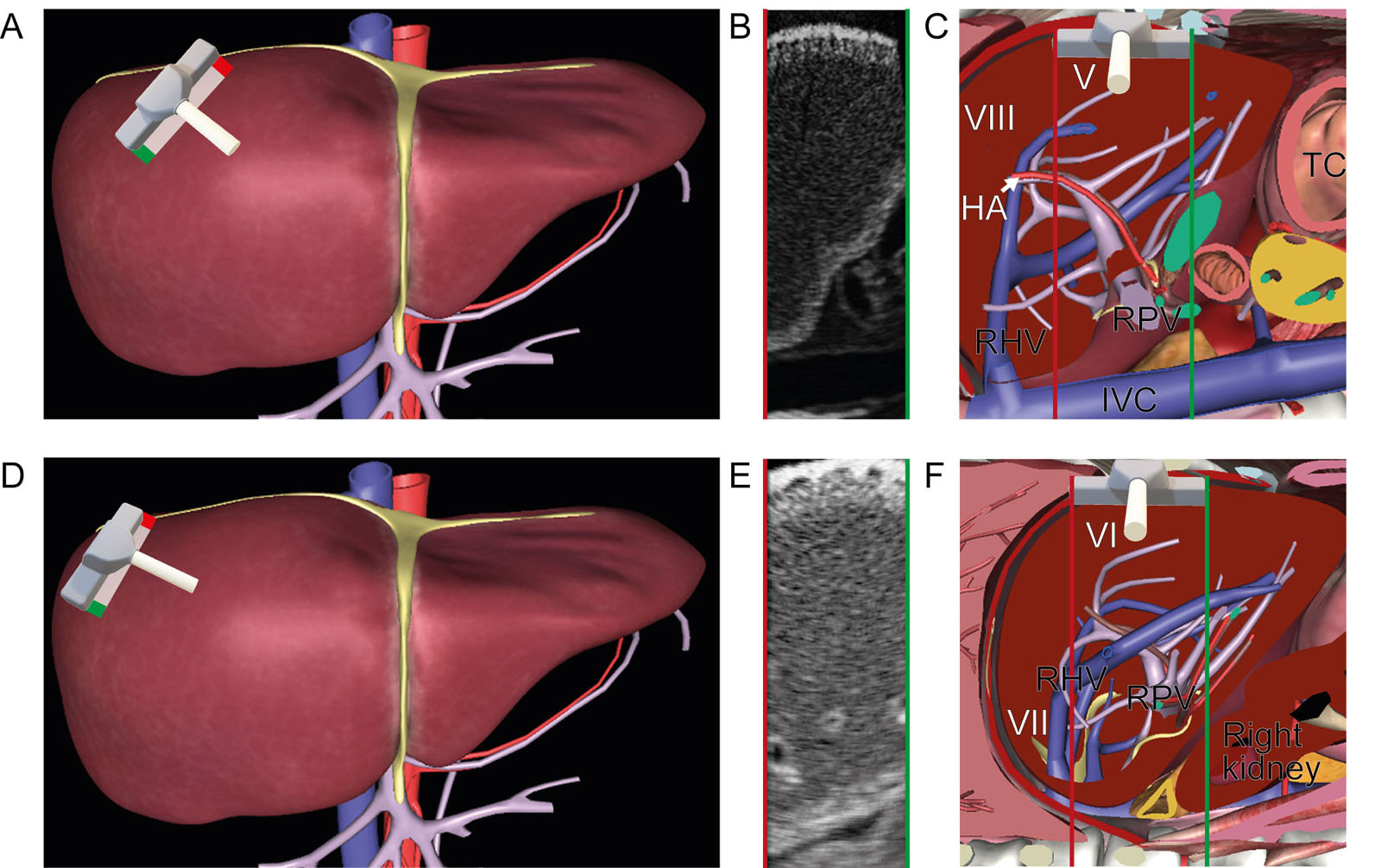
eFigure 28.9
Intraoperative right liver surface US scan. These are diagrams of a liver surface US examination of the right lobe of the liver using a linear probe. The right lobe divides into the RAS medial to the RHV and the RPS lateral to the RHV. These are the corresponding Couinaud segments (A-C) V and VIII in the RAS and (D-F) VI and VII in the RPS. Abbreviations: HA, hepatic artery; IVC, inferior vena cava; RAS, right anterior segment; RHV, right hepatic vein; RPS, right posterior segment; RPV, right portal vein; TC, transverse colon; US, ultrasound. (See Figure 28.2 for Couinaud segments identification)
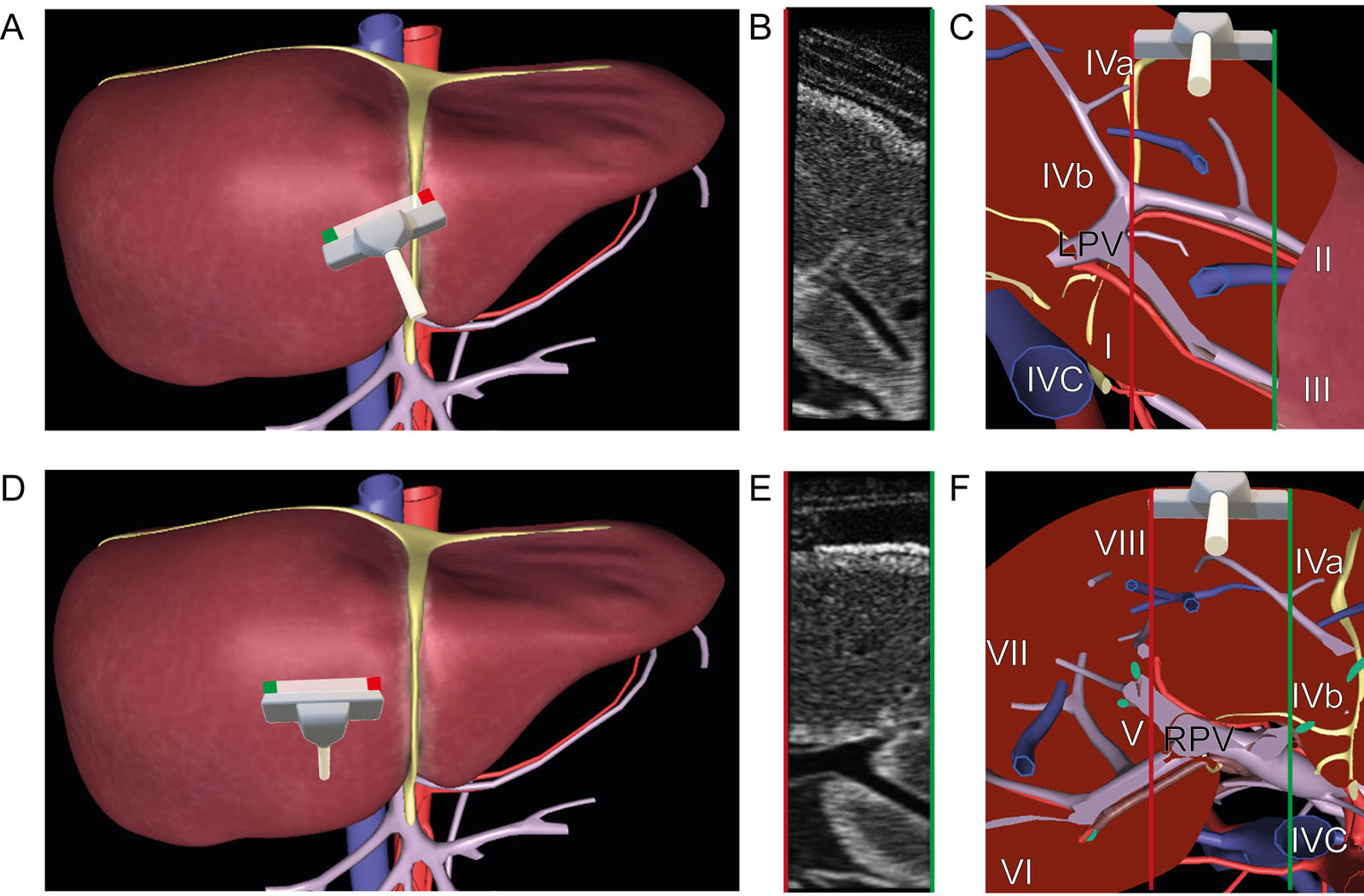
eFigure 28.10
Intraoperative left liver surface US scan. These are diagrams of a liver surface US examination of the left lobe of the liver using a linear probe. The left liver lobe divides into the LMS located between the MHV and the LHV and the LLS at the left of the LHV. The corresponding Couinaud segments (A-C) II and III in the LLS and (D-F) IVa and IVb in the LMS can be identified. Abbreviations: IVC, inferior vena cava; LHV, left hepatic vein; LLS, left lateral segment; LMS, left medial segment; LPV, left portal vein; MHV, middle hepatic vein; US, ultrasound.
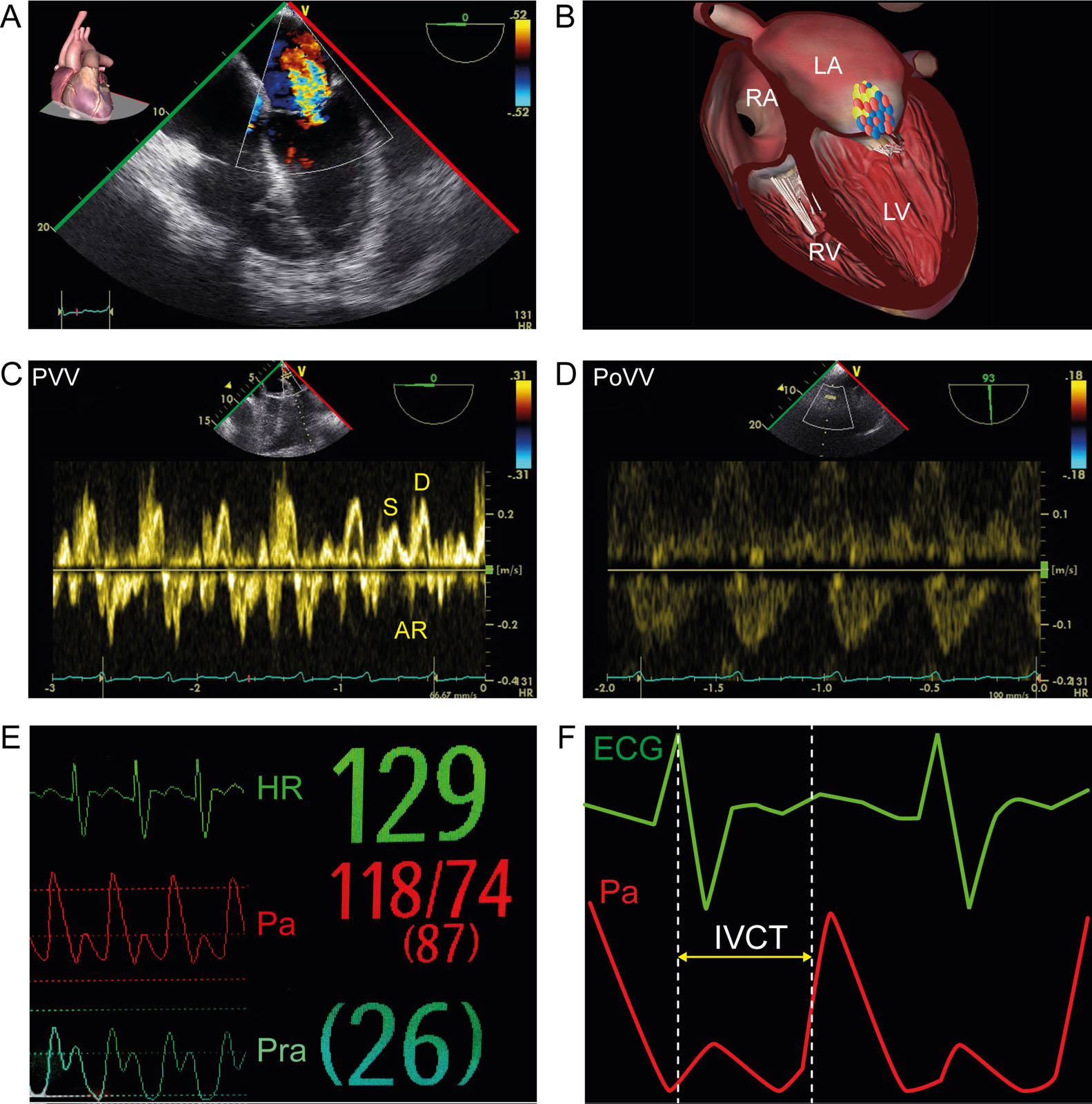
eFigure 28.18
Cirrhosis and cardiomyopathy. This is a 62-year-old man with morbid obesity and cirrhosis. (A, B) ME 4C view with CFI shows dilated cardiomyopathy and MR associated with (C) abnormal PVV and (D) biphasic portal pulsatility. (E, F) The delayed and slow rising systolic Pa (pulsus tardus) in relation to the ECG suggests LV dysfunction. The elevated right atrial pressure (Pra) is consistent with RV dysfunction and splanchnic congestion. Abbreviations: 4C, four-chamber; AR, atrial reversal PVV; CFI, color flow imaging; D, diastolic PVV; ECG, electrocardiogram; HR, heart rate; IVCT, isovolumic contraction time; LA, left atrium; LV, left ventricle; ME, mid-esophageal; MR, mitral regurgitation; Pa, arterial pressure; PoVV, portal venous velocity; Pra, right atrial pressure; PVV, pulmonary vein velocity; RA, right atrium; RV, right ventricle; S, systolic PVV.
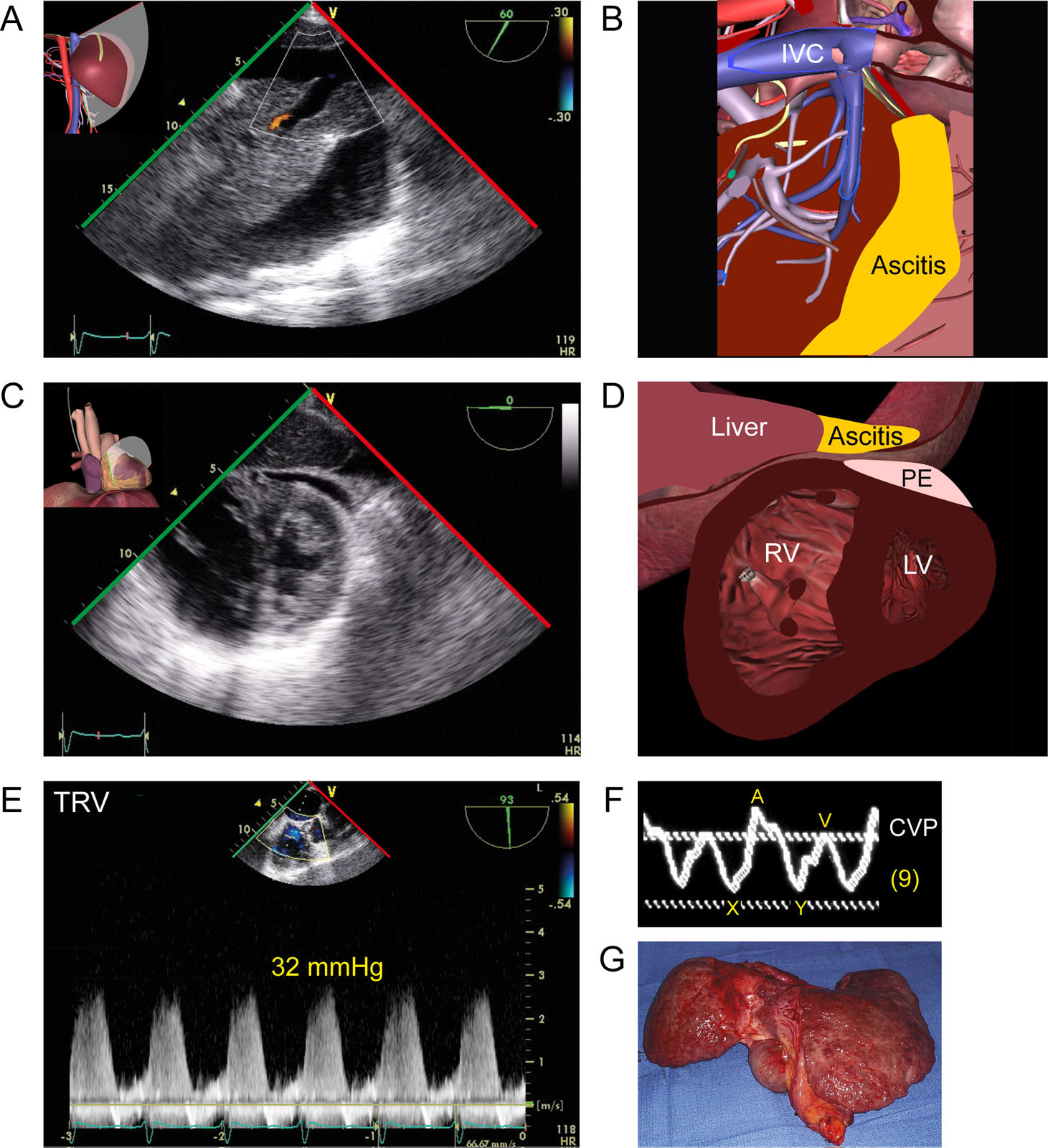
eFigure 28.19
Portopulmonary hypertension. This is a 73-year-old woman with cirrhosis and ascites. This is a (A,B) TGAUS view of the IVC and (C,D) mid-papillary TG view showing a D-shape RV, PE and ascites. (E) CWD across the tricuspid valve gives a TR peak pressure gradient of 32 mmHg, which added to the CVP, suggests elevated PA pressure. (F) Note the abnormal CVP waveform with elevated V wave and X and Y descent equalization. (G) Anatomical aspect of the cirrhotic liver. Abbreviations: CVP, central venous pressure; CWD, continuous wave Doppler; IVC, inferior vena cava LV, left ventricle; PA, pulmonary artery; PE, pericardial effusion; RV, right ventricle; TG, transgastric; TGAUS, transgastric abdominal ultrasound; TR, tricuspid regurgitation; TRV, tricuspid regurgitation velocity.
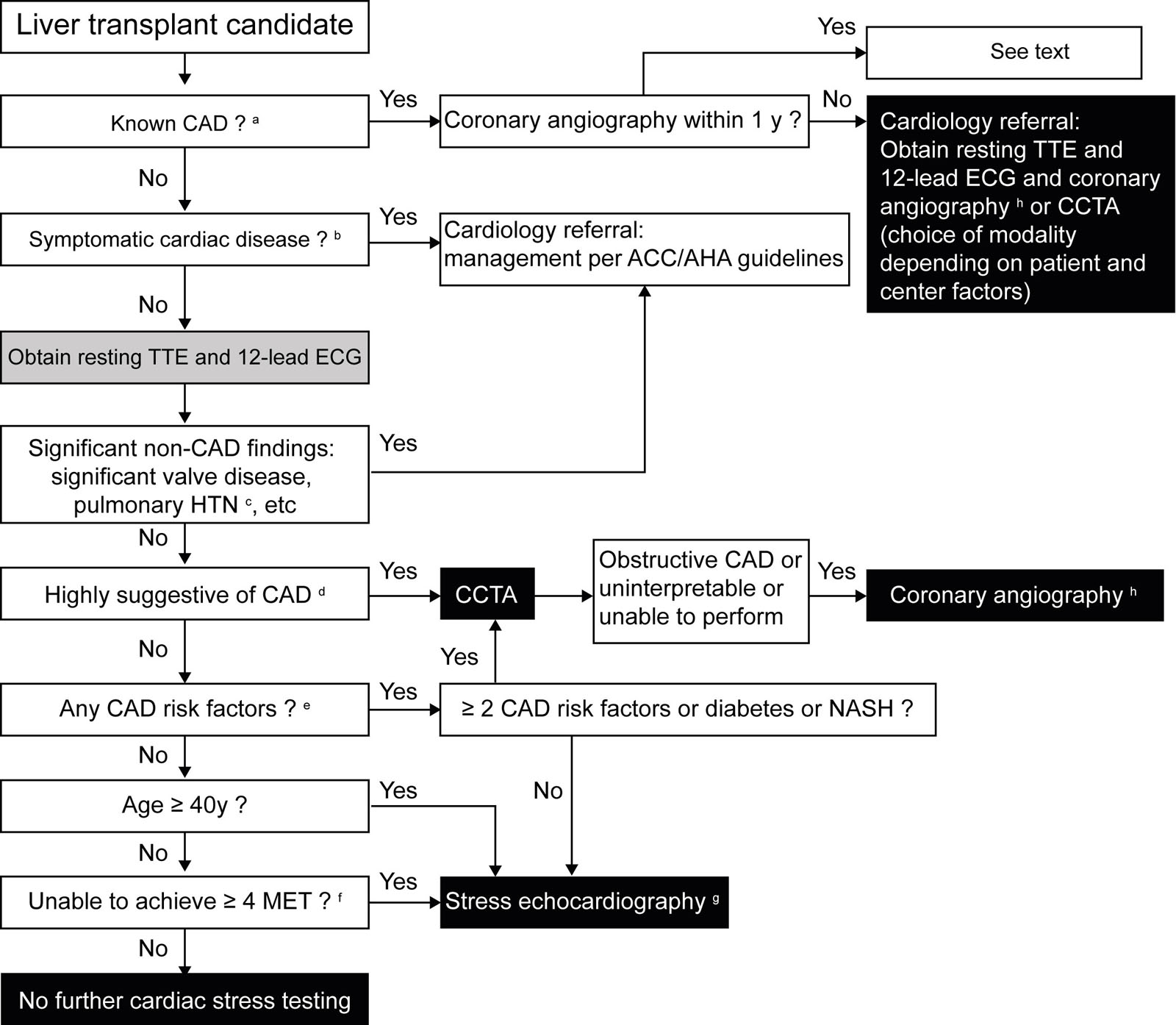
eFigure 28.21
Cardiac assessment pre-liver transplant. This algorithm represents an approach to CAD screening and risk stratification in liver transplantation candidates. aCHD is a history of MI, revascularization (CABG or PCI) or known >50% stenosis in a major epicardial coronary artery. bSymptomatic cardiac disease: angina, angina equivalent, or possible symptoms referrable to known CHF, arrhythmias, long QTc, or valvular disease. cPulmonary hypertension: in the absence of significant volume overload, RVSP >45 mmHg, RV dysfunction/hypertrophy, septal flattening, moderate tricuspid regurgitation, LVOTO, pericardial fluid and intracardiac shunt. dHighly suggestive of CAD: silent MI on ECG or TTE with new or unexpected regional LV RWMA or new or unexpected LV systolic (LVEF <50% or absolute LV GLS <18%). eCAD risk factors: dyslipidemia, history of HTN, chronic kidney disease, LVH, family history of premature CAD, active or past tobacco use, and coronary artery calcification score >0. fAt ≥4 METs, patients can climb ≥1 flights of stairs without stopping, walk up a hill for ≥1 to 2 blocks, scrub floors, move furniture, golf, dance, run, or play tennis. g Exercise SE preferred or dobutamine SE if the patient cannot exercise. Consider cardiac PET as an alternative if available. In patients whose critical illness precludes SE, consider CCTA or coronary angiography (depends on patient and center factors). hCoronary angiography: is the last test before the patient listing and requires a multidisciplinary discussion of management plan if there is significant obstructive CAD. Abbreviations: ACC, American College of Cardiology; AHA, American Heart Association; CABG, coronary artery bypass grafting; CCTA, coronary computed tomography angiography; CAD, coronary heart disease; CCTA, coronary computed tomography; CHD, coronary heart disease; CHF, congestive heart failure; ECG, electrocardiogram; GLS, global longitudinal strain; HTN, hypertension; LV, left ventricular; LVEF, left ventricular ejection fraction; LVH, left ventricular hypertrophy; LVOTO, left ventricular outflow tract obstruction; MET, metabolic equivalent; MI, myocardial infarction; NASH, nonalcoholic steatohepatitis; PCI, percutaneous coronary intervention; PET, positron emission tomography; RV, right ventricular; RVSP, right ventricular systolic pressure; RWMA, regional wall motion abnormality; SE, stress echocardiography; TTE, transthoracic echocardiogram. Adapted from Raval36 and Cheng et al.41
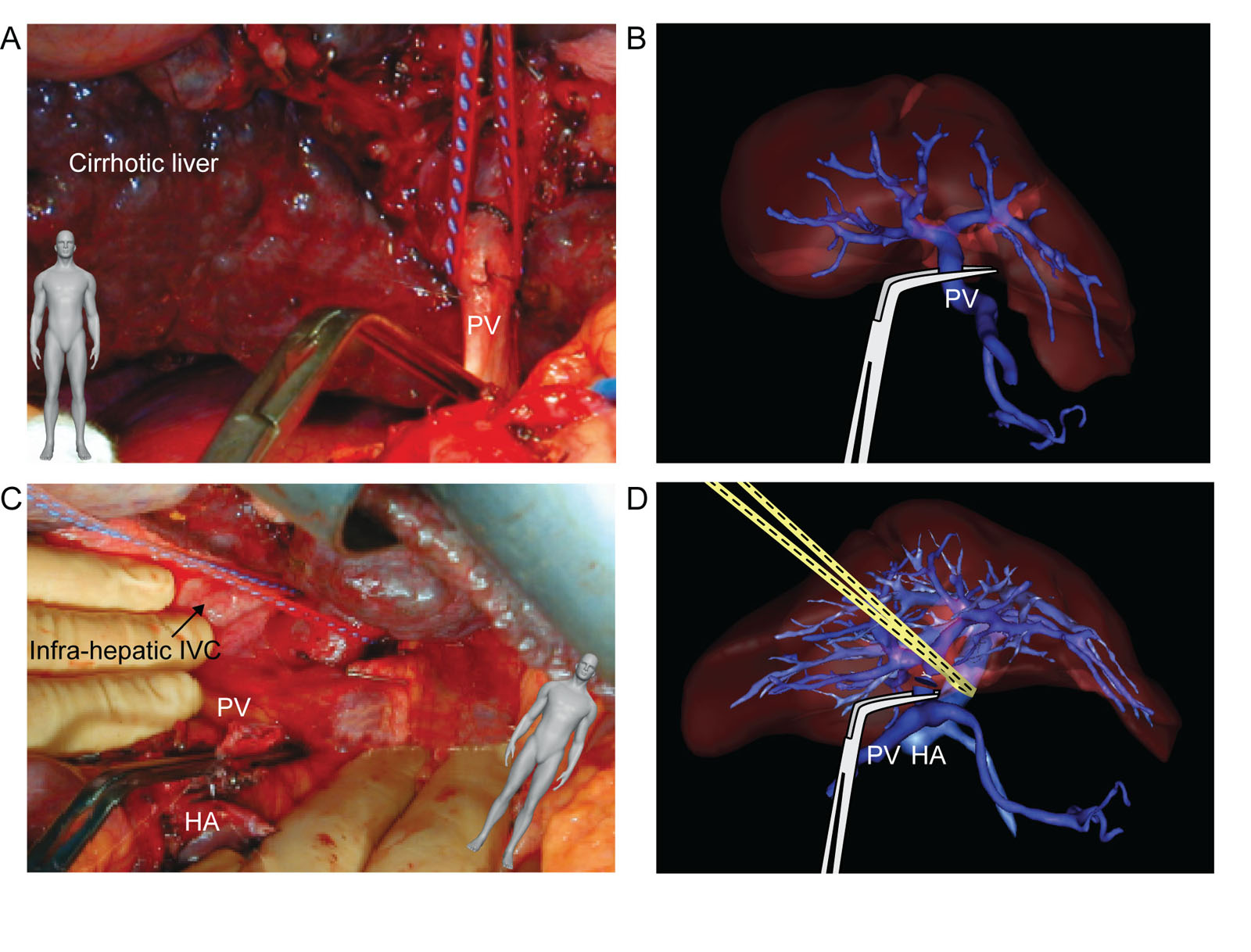
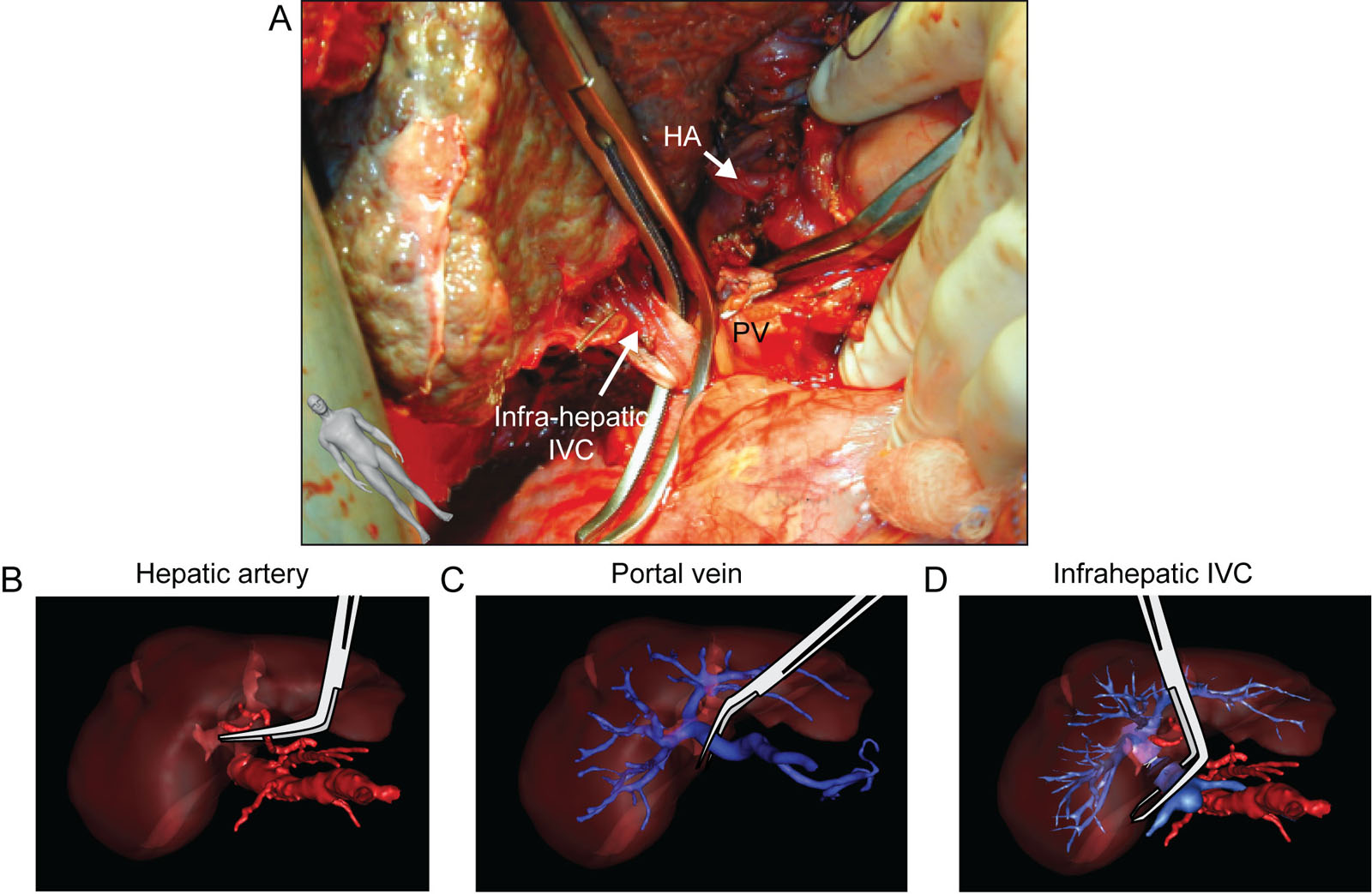
eFigure 28.23
Liver transplant portal vein. These surgical photos and 3D reconstruction diagrams show (A,B) PV identification and clamping, as well as (C,D) hepatic vasculature during liver transplantation. Abbreviations: 3D, three-dimensional; HA, hepatic artery; IVC, inferior vena cava; PV, portal vein. Part B and D courtesy of the Institut de Recherche Contre les Cancers de I’Appareil Digestif, Strasbourg, France.
eFigure 28.24
Liver transplant infrahepatic IVC. (A) This surgical photo shows the dissection and clamping of the infrahepatic IVC and PV during liver transplantation. (B–D) These are the corresponding 3D reconstruction during the clamping of the major hepatic vessels. Abbreviations: 3D, three-dimensional; HA, hepatic artery; IVC, inferior vena cava; PV, portal vein. Source: Parts B to D courtesy of the Institut de Recherche Contre les Cancers de l’Appareil Digestif, Strasbourg, France.
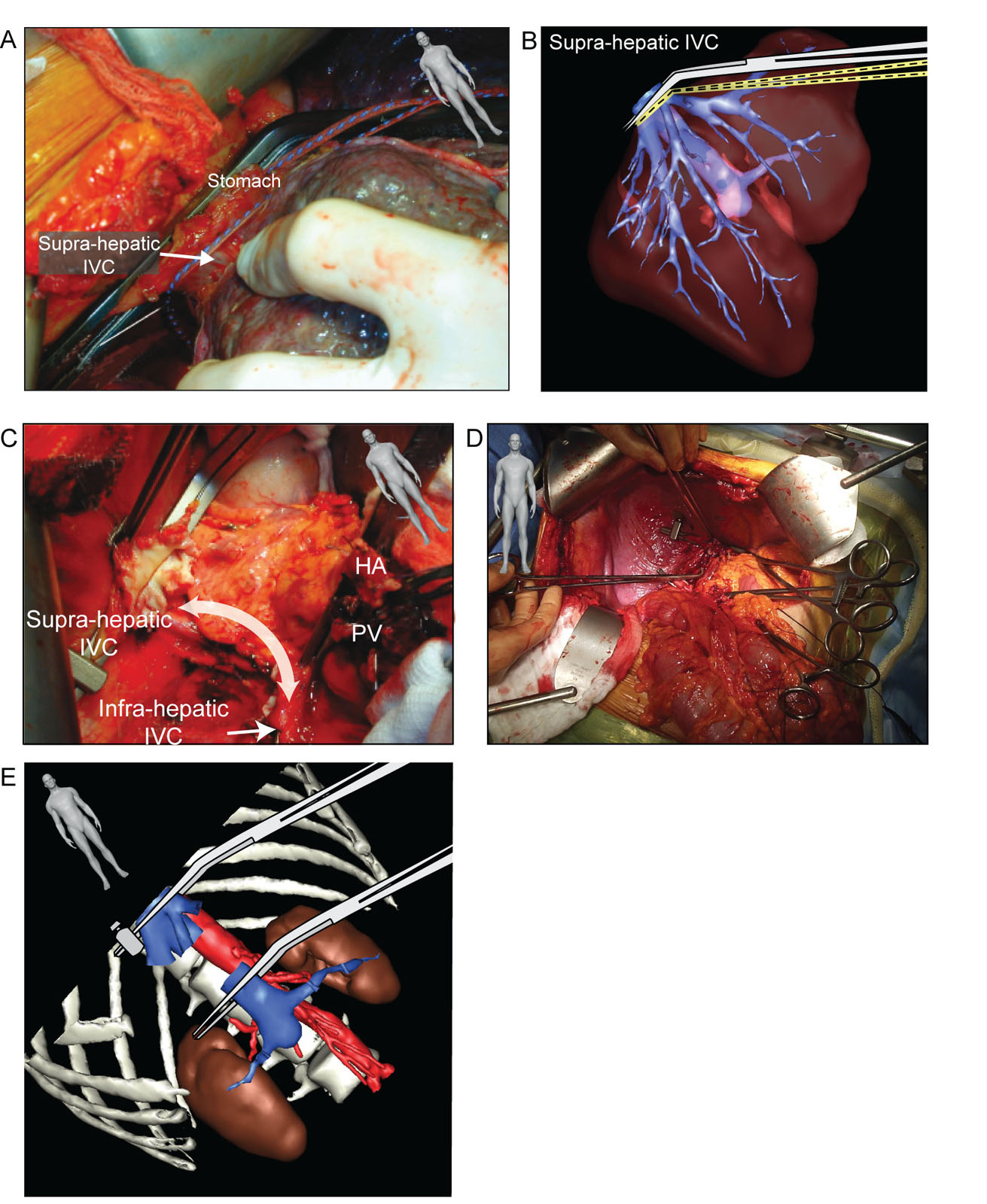
eFigure 28.25
Liver transplant suprahepatic IVC. These surgical photos and 3D reconstruction diagrams show (A,B) the dissection and clamping of the suprahepatic IVC during orthotopic liver transplantation.These intraoperative photos show (C) the residual supra- and infrahepatic IVC after removing the liver and (D) the retrohepatic IVC portion during the anhepatic phase with the (E) corresponding 3D reconstruction. Abbreviations: 3D, three-dimensional; HA, hepatic artery; IVC, inferior vena cava; PV, portal vein. Source: Part B and E courtesy of the Institut de Recherche Contre les Cancers de l’Appareil Digestif, Strasbourg, France.
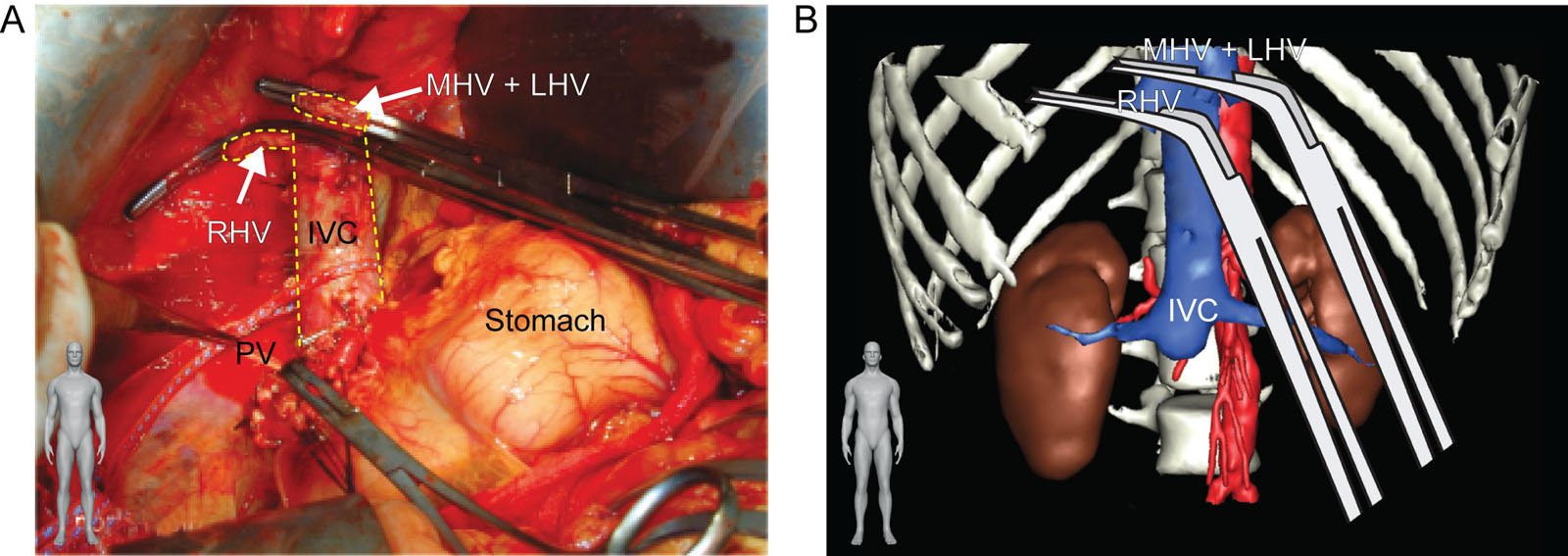
eFigure 28.26
Liver transplant piggy-back technique. This is a (A) surgical photo and (B) 3D reconstruction during the anhepatic phase of a liver transplant using the piggy-back technique. The intraoperative photo shows the remaining intact retrohepatic IVC after removing the liver at the hepatic vein level. Abbreviations: 3D, three-dimensional; IVC, inferior vena cava; LHV, left hepatic vein; MHV, middle hepatic vein; PV, portal vein; RHV, right hepatic vein. Source: Part B courtesy of the Institut de Recherche Contre les Cancers de l’Appareil Digestif, Strasbourg, France.
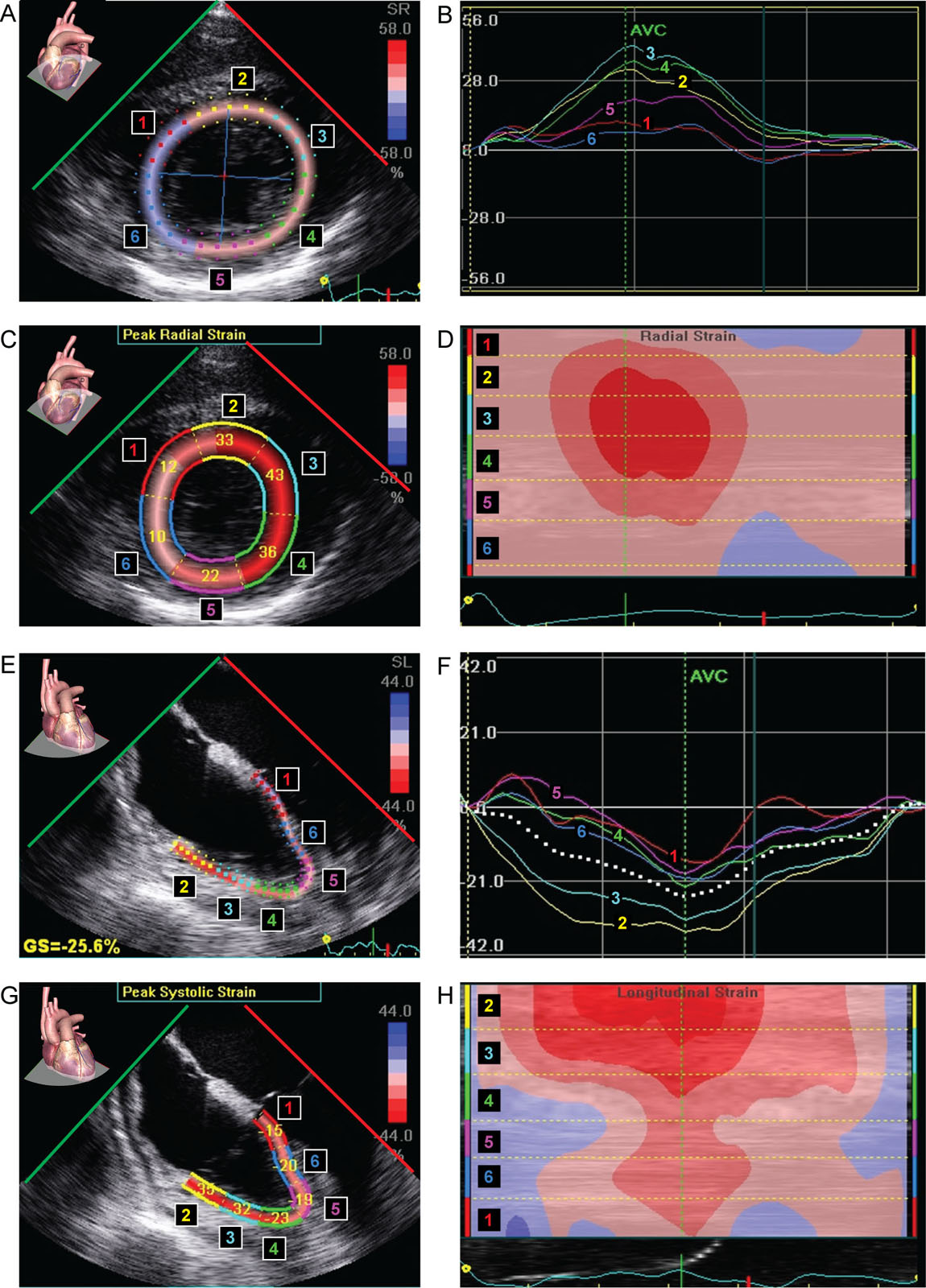
eFigure 28.34
LV and RV strain. This is a 72-year-old man after a liver transplantation. (A-D) LV peak radial strain and (E-H) RV global longitudinal strain both have regional strain abnormalities. Abbreviations: AVC, aortic valve closure; GS, global strain; LV, left ventricular; RV, right ventricular.
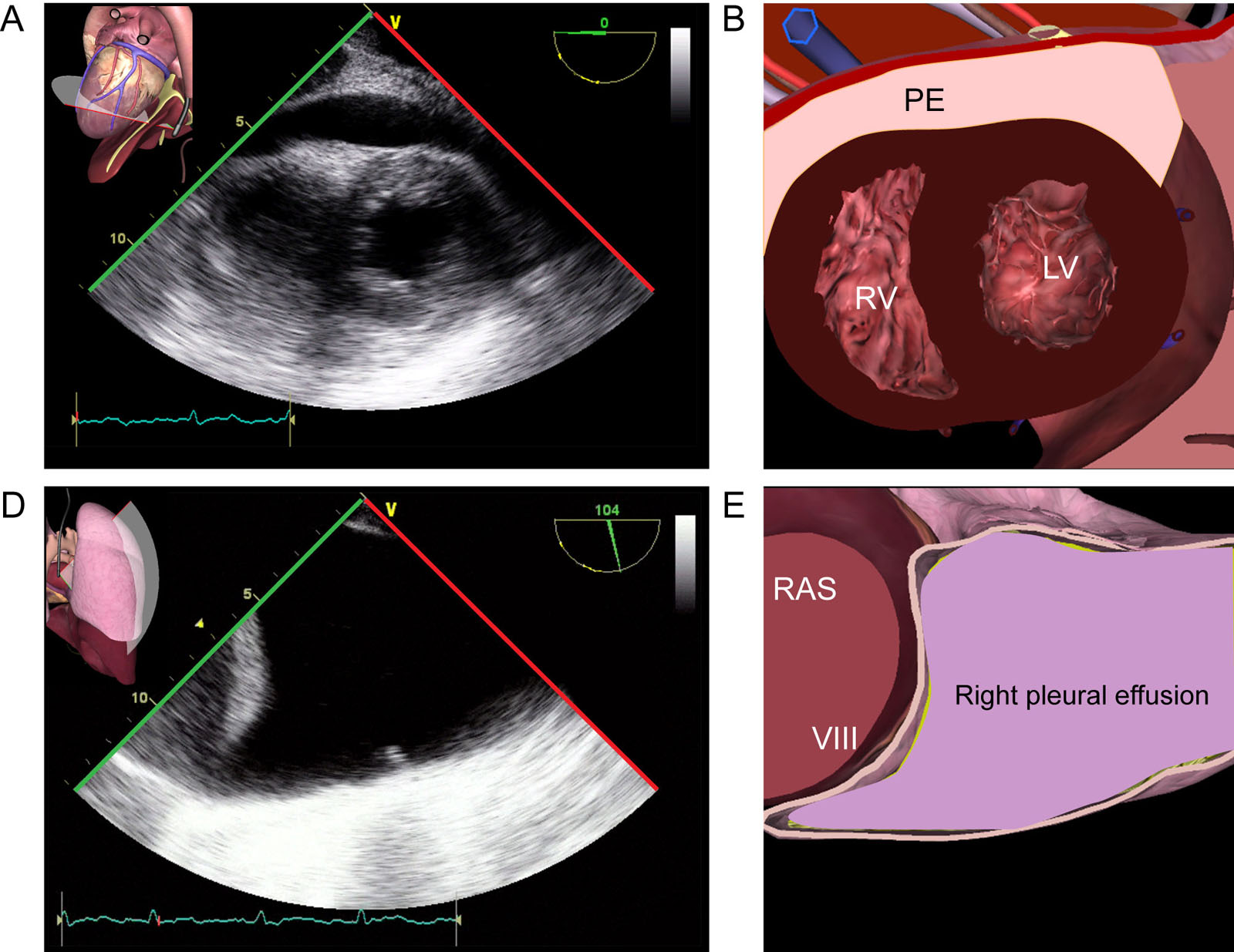
eFigure 28.40
Pericardial and pleural effusions. This is a 72-year-old man who became hemodynamically unstable after liver transplantation. (A,B) TG apical view shows a posterior PE. (C,D) A right pleural effusion is also present on TELUS. Abbreviations: LV, left ventricle; PE, pericardial effusion; RAS, right anterior sector; RV, right ventricle; TELUS, transesophageal lung ultrasound; TG, transgastric.
Videos
Chapter 28 Fig02A
Chapter 28 Fig03AB
Chapter 28 Fig05A
Chapter 28 Fig06
Chapter 28 Fig12A
Chapter 28 Fig12B
Chapter 28 Fig12C
Chapter 28 Fig13A
Chapter 28 Fig13C
Chapter 28 Fig14A
Chapter 28 Fig14D
Chapter 28 Fig15A
Chapter 28 Fig15D
Chapter 28 Fig16A_1
Chapter 28 Fig16A
Chapter 28 Fig16C
Chapter 28 Fig17A
Chapter 28 Fig17C
Chapter 28 Fig18A
Chapter 28 Fig19A
Chapter 28 Fig19C
Chapter 28 Fig20A
Chapter 28 Fig20B
Chapter 28 Fig23AB
Chapter 28 Fig24A
Chapter 28 Fig25ABCDE
Chapter 28 Fig26A
Chapter 28 Fig29AC
Chapter 28 Fig29D
Chapter 28 Fig30AC
Chapter 28 Fig31DE
Chapter 28 Fig33D
Chapter 28 Fig34A
Chapter 28 Fig34E
Chapter 28 Fig35A
Chapter 28 Fig35D
Chapter 28 Fig37A
Chapter 28 Fig37D
Chapter 28 Fig38B
Chapter 28 Fig38C
Chapter 28 Fig39A
Chapter 28 Fig39EF
Chapter 28 Fig40A
Chapter 28 Fig40D
Tables
eTable 28.1 TEE views for liver transplantation rescue TEE
Icon |
View-Technique |
Role |
|||
 |
ME 4C |
|
|||
 |
ME LAX |
|
|||
 |
ME RV Inflow-Outflow |
|
|||
 |
ME Bicaval |
|
|||
 |
TGAUS #4 |
|
|||
Abbreviations: 4C, four-chamber; AoV, aortic valve; CPR, cardiopulmonary resuscitation; IAS, interatrial septum; IVC, inferior vena cava; IVS, interventricular septum; LAX, long-axis; LHV, left hepatic vein; LV, left ventricle; LVOTO, left ventricular outflow tract obstruction; ME, mid-esophageal; MHV, middle hepatic vein; MV, mitral valve; PA, pulmonary artery; PV, pulmonic valve; RHV, right hepatic vein; RV, right ventricle; RVOTO, right ventricular outflow tract obstruction; SVC, superior vena cava; TEE, transesophageal echocardiography; TGAUS, transgastric abdominal ultrasound; TV, tricuspid valve; WMA, wall motion abnormalities. Adapted from Vanneman et al.79 |
|||||