Figures
eFigure 30.5
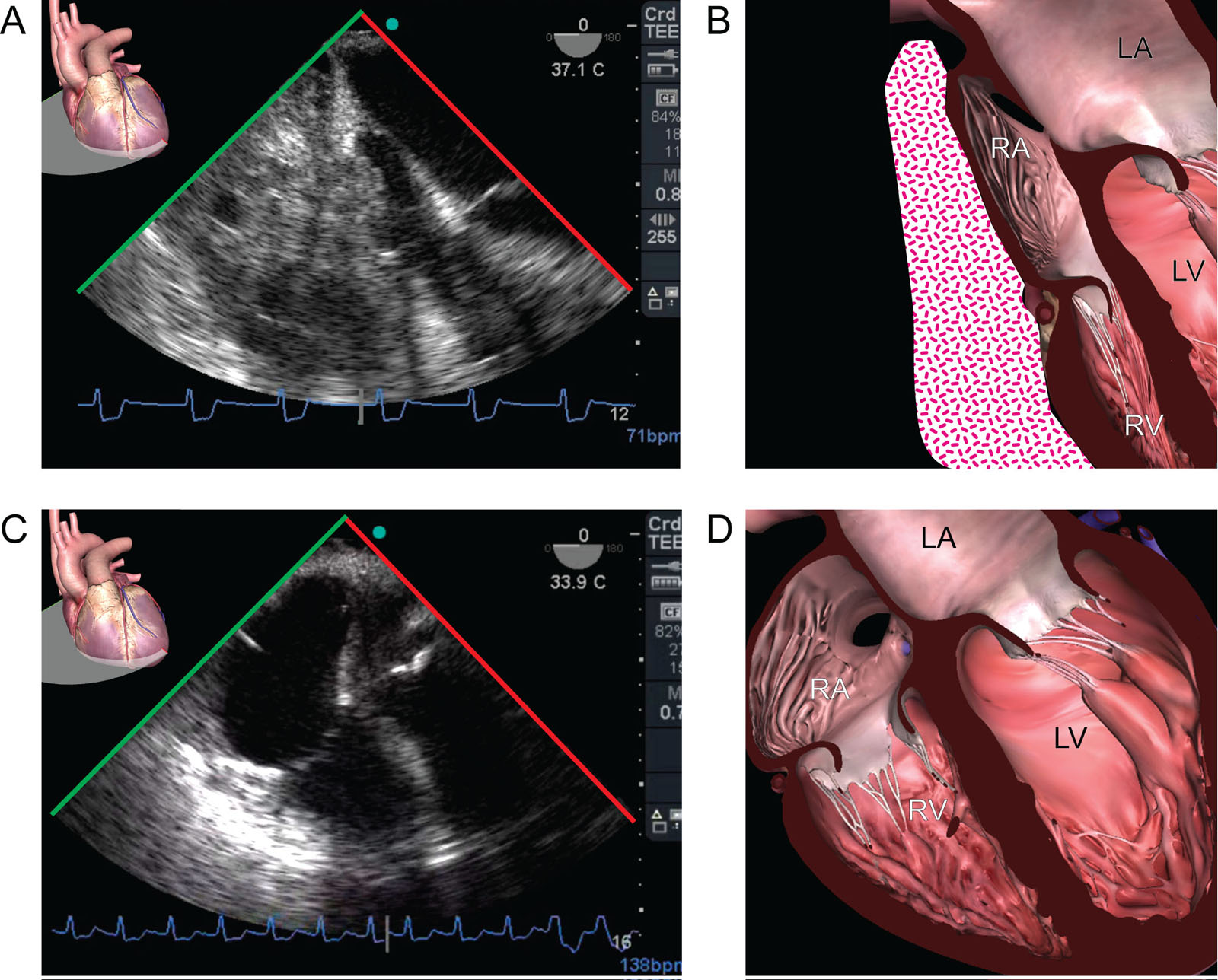
Cardiac tamponade. This is a hemodynamically unstable 68-year-old woman after cardiac surgery. (A, B) ME 4C view shows a clot compressing the RA and RV. (C, D) The right heart chambers expand after clot evacuation. Abbreviations: 4C, four-chamber; LA, left atrium; LV, left ventricle; ME, mid-esophageal; RA, right atrium; RV, right ventricle. Adapted from Durand et al.210
eFigure 30.6
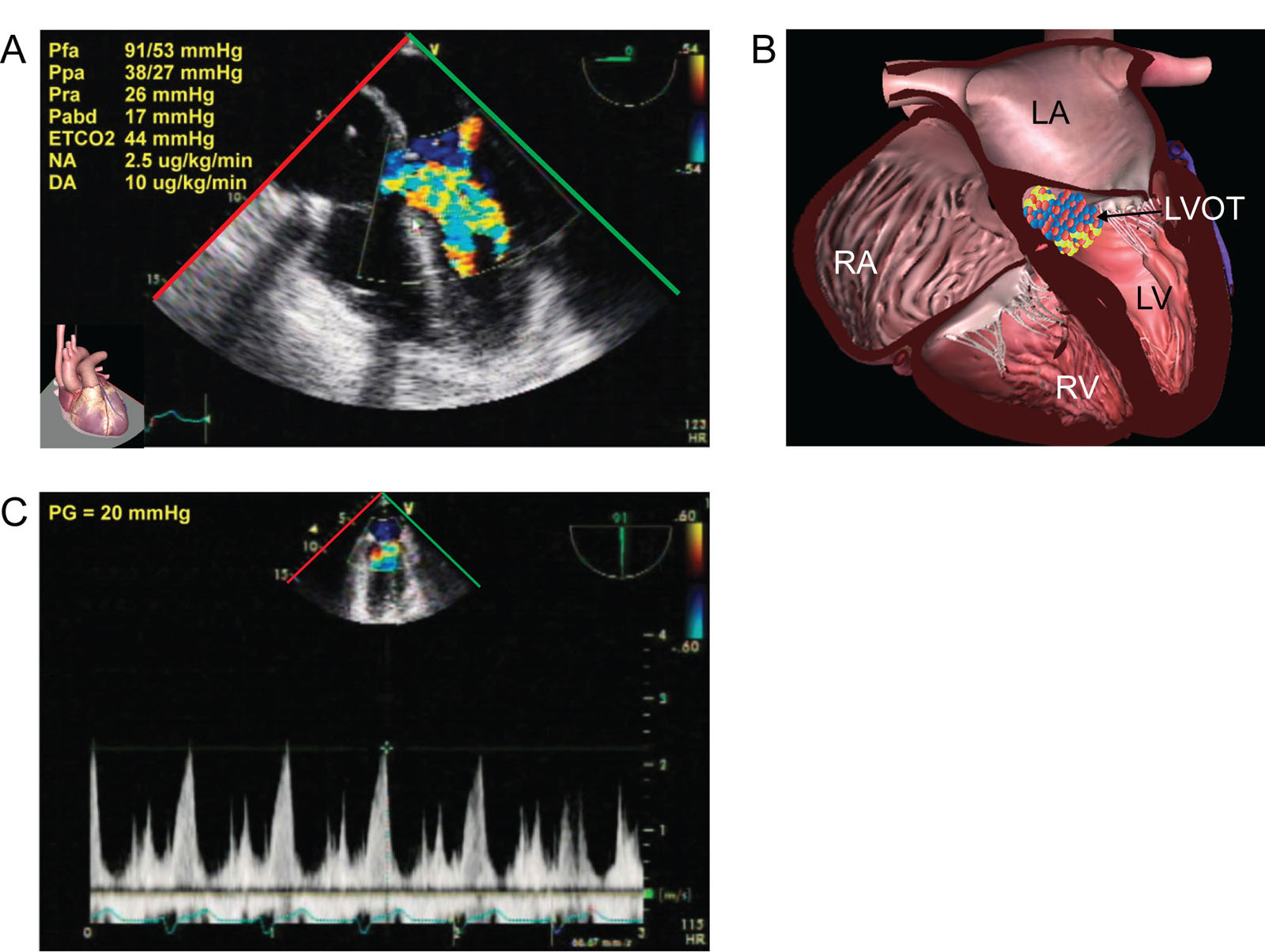
Dynamic LVOTO. This is a 47-year-old man following cardiac arrest from RCA occlusion. (A, B) ME 5C view with CFI shows flow acceleration in the LVOT consistent with SAM. (C) CWD of the LVOT gives a late-peaking systolic gradient of 20 mmHg after treatment. The cause of the LVOTO was perhaps both inotrope usage and RV dysfunction from the RCA occlusion. Abbreviations: 5C, five-chamber; CFI, color flow imaging; CWD, continuous wave Doppler; DA, dopamine; ETCO2, end-tidal CO2; LA, left atrium, LV, left ventricle; LVOT, left ventricular outflow tract; LVOTO, left ventricular outflow tract; ME, mid-esophageal; Pabd, abdominal pressure; Pfa, femoral arterial pressure; PG, pressure gradient; Ppa, pulmonary artery pressure; Pra, right atrial pressure; RA, right atrium; RCA, right coronary artery; RV, right ventricle; SAM, systolic anterior motion.
eFigure 30.7
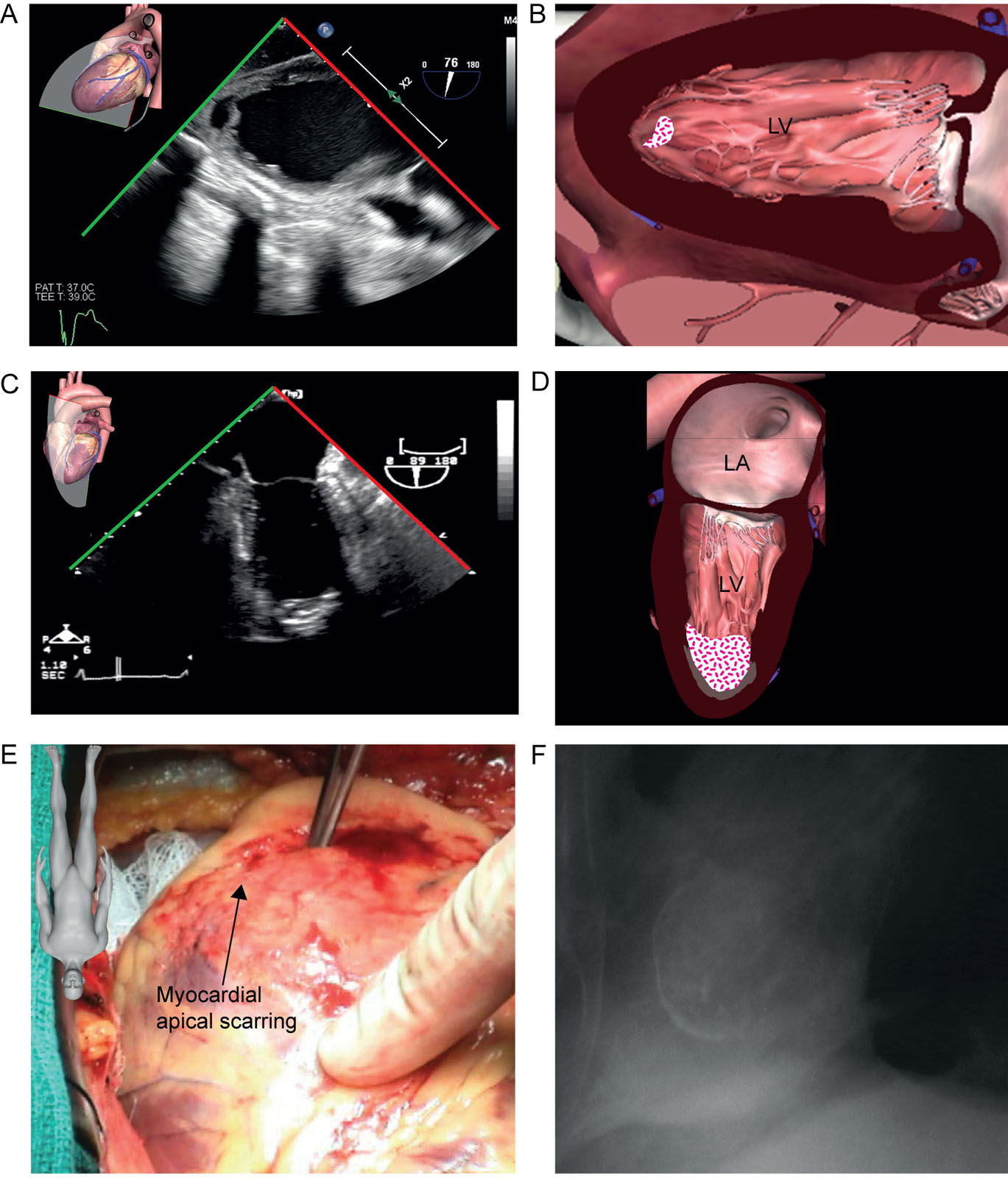
LV apical thrombus. (A, B) This is a 35-year-old man with cardiomyopathy evaluated for LVAD. The TG 2C view shows an unexpected mobile apical LV thrombus (arrow). (C, D) This is a 79-year-old man with a prior anterior myocardial infarction. (C) The ME 2C view shows a calcified apical thrombus which (D) intraoperatively was under the calcified scar. (E) The lateral chest X-ray shows the calcified aneurysm. Abbreviations: 2C, two-chamber; LA, left atrium; LV, left ventricle; LVAD, left ventricular assist device; ME, mid-esophageal; TG, transgastric. Source: Photo A and E courtesy of Dr. JK Shim and Dr. Raymond Cartier.
eFigure 30.10
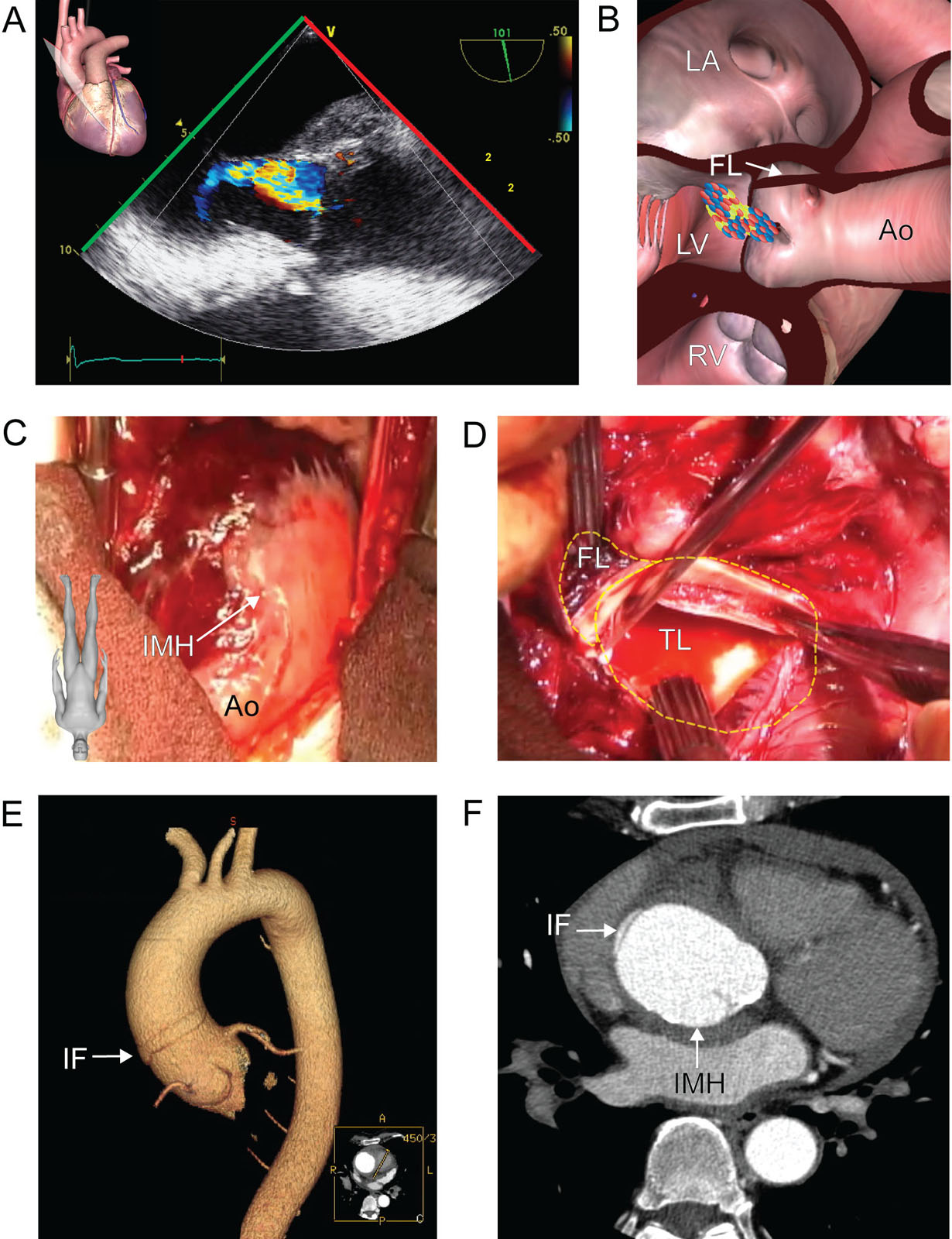
Acute aortic dissection. This is a hemodynamically stable patient with known AR who is presented to the emergency room with acute chest pain radiating to the back. (A, B) ME AoV LAX view with CFI shows eccentric moderate AR directed toward the AMVL from a prolapsed right coronary cusp. (C, D) These are the intraoperative photos (C) before and (D) after Asc Ao opening just above a visible IMH. (E, F) CT shows the hematoma and an intimal flap 2 cm above the origin of the right coronary artery. Abbreviations: AMVL, anterior mitral valve leaflet; Ao, aorta; AoV, aortic valve; AR, aortic regurgitation; Asc Ao, ascending aorta; CFI, color flow imaging; CT, computed tomography; FL, false lumen; IF, intimal flap; IMH, intramural hematoma; LA, left atrium; LAX, long-axis; LV, left ventricle; ME, mid-esophageal; RV, right ventricle; TL, true lumen. Source: Courtesy of Drs. Michel Carrier and Carl Chartrand-Lefebvre.
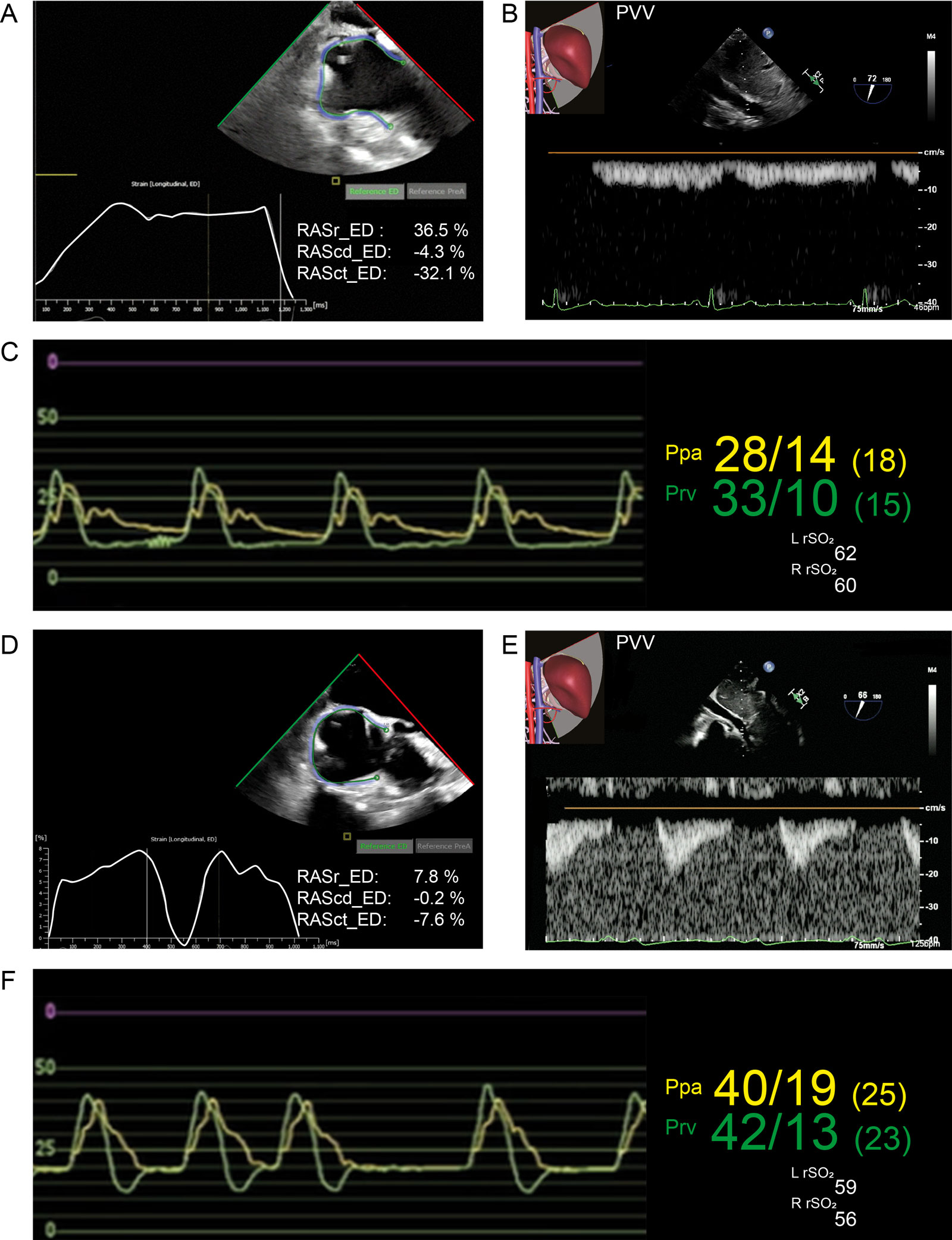
eFigure 30.14
RA strain, portal pulsatility and fluid responsiveness. (A) RA strain before coronary revascularization surgery was 36%. After CPB, there was (B) monophasic portal vein velocity by PWD, (C) normal RV pressure waveform and (D) reduced RA strain at 7.8%. Transfusion of 200 ml blood resulted in (E) significant portal pulsatility and (F) increased Ppa and Prv pressure with a square root sign and reduction in rSO2 suggesting liver and brain venous congestion. Abbreviations: CPB, cardiopulmonary bypass; ED, end-diastole; L, left; Ppa, pulmonary artery pressure; Prv, right ventricular pressure; PVV, portal vein velocity; R, right; RA, right atrial; RAScd, right atrial conduit strain; RASct, right atrial contraction strain; RASr, right atrial strain reservoir; rSO2, regional oxygen cerebral saturation; RV, right ventricular.
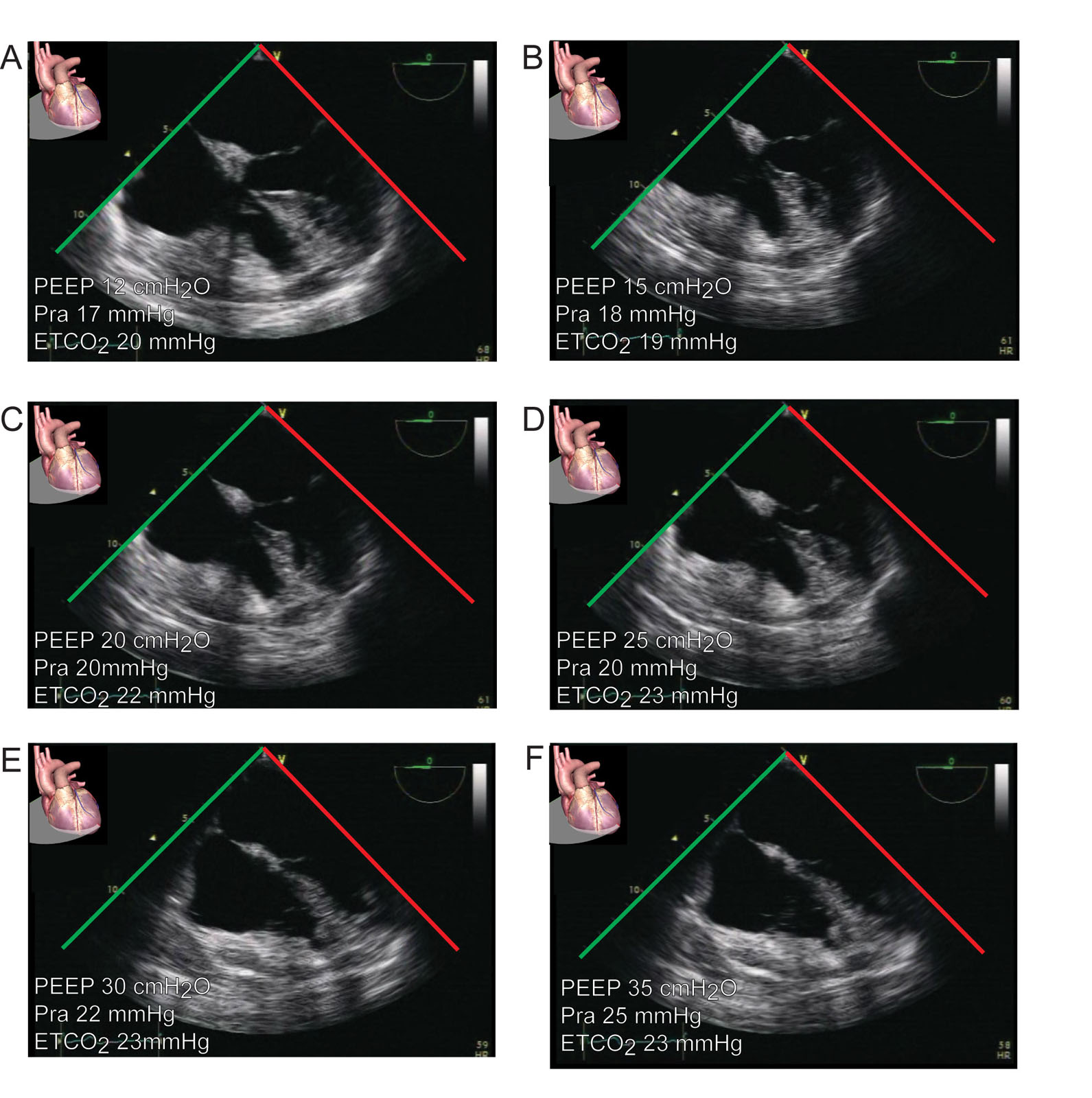
eFigure 30.20
Lung recruitment. This is a 75-year-old woman with acute hypoxic respiratory failure. (A–F) ME 4C views show changes in RA and RV size as PEEP increases from 12 to 30 cmH2O, escalating Pra from 17 to 25 mmHg and ETCO2 to a maximum of 23 mmHg at 25 cmH2O of PEEP. Abbreviations: 4C, four-chamber; ETCO2, end-tidal carbon dioxide; ME, mid-esophageal; PEEP, positive end-expiratory pressure; Pra, right atrial pressure; RA, right atrium; RV, right ventricle.
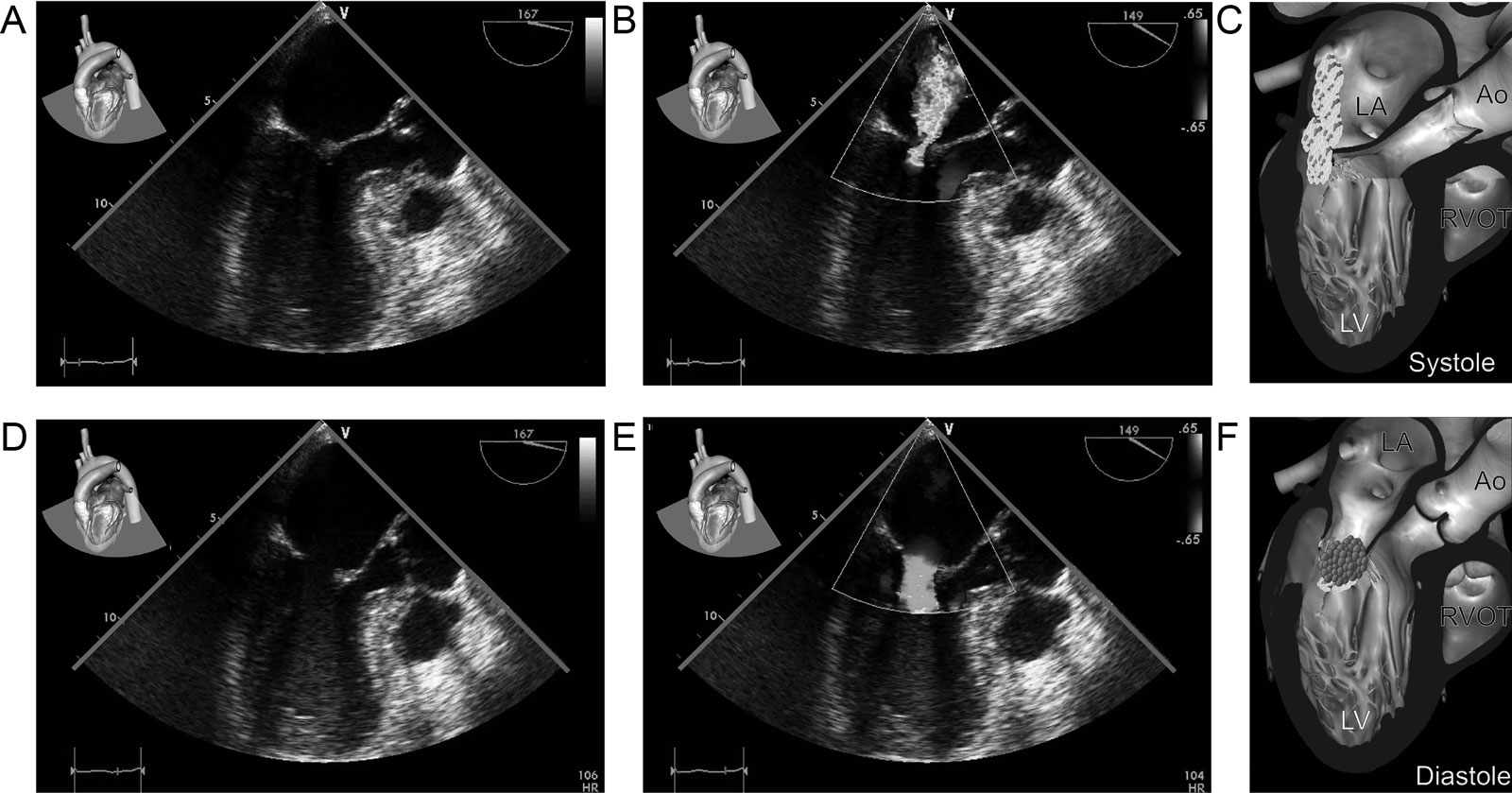
eFigure 30.22
Takotsubo syndrome. This patient receiving intravenous adrenaline developed (A-F) apical akinesia associated with mild MR in the ME LAX view with CFI that resolved after stopping the adrenaline. Abbreviations: Ao, aorta; CFI, color flow imaging; LA, left atrium; LAX, long-axis view; LV, left ventricle; ME, mid-esophageal; MR, mitral regurgitation; RVOT, right ventricular outflow tract.
Videos
Chapter 30 Fig03A
Chapter 30 Fig03C
Chapter 30 Fig05A
Chapter 30 Fig05C
Chapter 30 Fig07A
Chapter 30 Fig07C
Chapter 30 Fig07E
Chapter 30 Fig08A
Chapter 30 Fig09A
Chapter 30 Fig09D
Chapter 30 Fig10A
Chapter 30 Fig10C
Chapter 30 Fig10D
Chapter 30 Fig11A
Chapter 30 Fig14AC
Chapter 30 Fig14D
Chapter 30 Fig14F
Chapter 30 Fig15A
Chapter 30 Fig15B
Chapter 30 Fig15C
Chapter 30 Fig15D
Chapter 30 Fig16B
Chapter 30 Fig16E
Chapter 30 Fig17B
Chapter 30 Fig18B
Chapter 30 Fig18D
Chapter 30 Fig20A
Chapter 30 Fig20F
Chapter 30 Fig21A
Chapter 30 Fig21B
Chapter 30 Fig21C
Chapter 30 Fig21D
Chapter 30 Fig21E
Chapter 30 Fig21F
Chapter 30 Fig21G
Chapter 30 Fig21H
Chapter 30 Fig22A
Chapter 30 Fig22B
Tables
eTable 30.2 Diagnostic criteria for stress cardiomyopathy*
|
* according to the Heart Failure Association of the European Society of Cardiology diagnostic criteria for Takotsubo Syndrome |
a Acute, reversible dysfunction of a single coronary territory has been reported |
Abbreviations: BNP, b-type natriuretic peptide; ECG, electrocardiography; LBBB, left bundle branch block; LV, left ventricular; NT-proBNP, N-terminal pro b-type natriuretic peptide; RV, right ventricular; RWMA, regional wall motion abnormality. Adapted from Lyon et al. 178 |