Figures
Videos
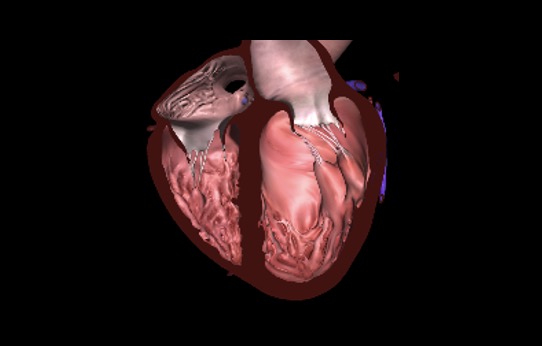
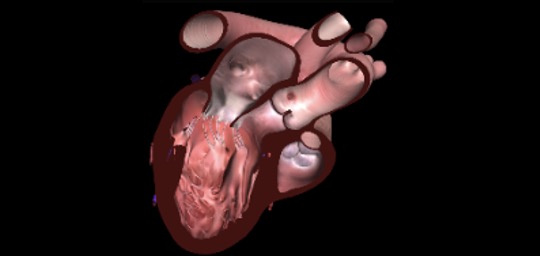
Chapter 31 Fig01A
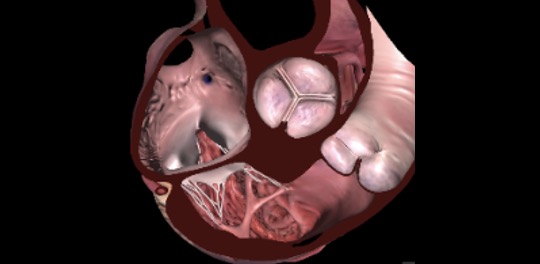
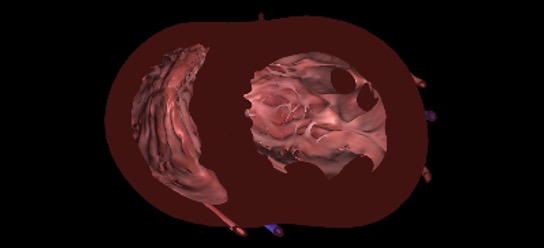
Chapter 31 Fig01C
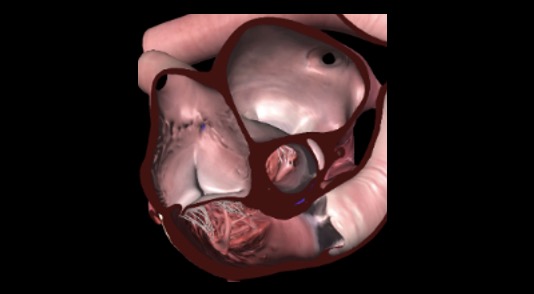
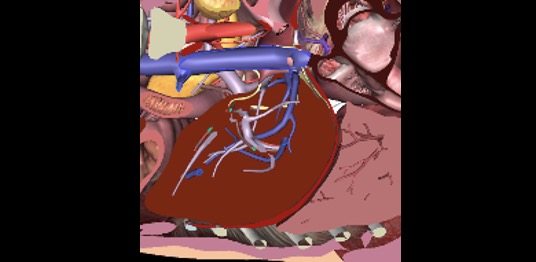
Chapter 31 Fig01E
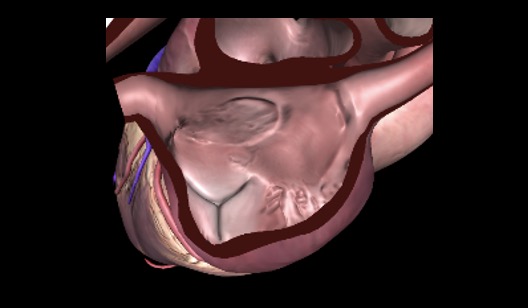
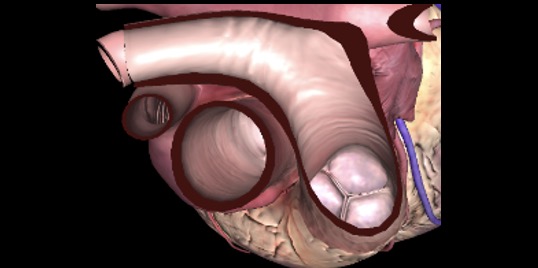
Chapter 31 Fig01G
Chapter 31 Fig03AC
Chapter 31 Fig03E
Chapter 31 Fig04A
Chapter 31 Fig04C
Chapter 31 Fig05A
Chapter 31 Fig05C
Chapter 31 Fig05D
Chapter 31 Fig06A
Tables
eTable 31.4. TEE evaluation post ROSC: TEE extended views, TELUS and TGAUS
|
TEE View |
View-Technique |
Role |
1 |
 |
ME 4C |
|
2 |
 |
ME AoV SAX |
|
3 |
 |
ME RV Inflow-Outflow |
|
4 |
 |
ME 2C |
|
5 |
 |
ME Bicaval |
|
6 |
 |
ME LAX |
|
7 |
 |
TG Mid papillary SAX |
|
8 |
 |
TGAUS LAX IVC |
|
9 |
 |
Descending aorta SAX |
|
10 |
 |
ME Ascending Aorta SAX |
|
11 |
 |
TELUS |
|
12 |
 |
TGAUS |
|
Abbreviations: 2C, two-chamber; 4C, four-chamber; AoV, aortic valve; CFI, color flow imaging; CVP, central venous pressure; ECPR, extracorporeal cardiopulmonary resuscitation; IABP, intra-aortic balloon pump; IAS, interatrial septum; IVC, inferior vena cava; IVS, interventricular septum; LAA, left atrial appendage; LAX, long-axis; LV, left ventricle; LVOT, left ventricular outflow tract obstruction; LVOTO, left ventricular outflow tract obstruction; ME, mid-esophageal; MV, mitral valve; PA, pulmonary artery; PV, pulmonic valve; REBOA; resuscitative endovascular balloon occlusion of the aorta; ROSC, return of spontaneous circulation; RV, right ventricle; RWMA, right wall motion abnormality; SAM, systolic anterior motion of mitral valve; SAX, short-axis; SVC, superior vena cava; TEE, transesophageal echocardiography; TELUS, transesophageal lung ultrasonography; TG, transgastric; TGAUS, transgastric abdominal ultrasonography; TV, tricuspid valve, VeXUS, venous access ultrasound. Adapted from Riendeau-Beaulac et al.9 |
|||