Figures
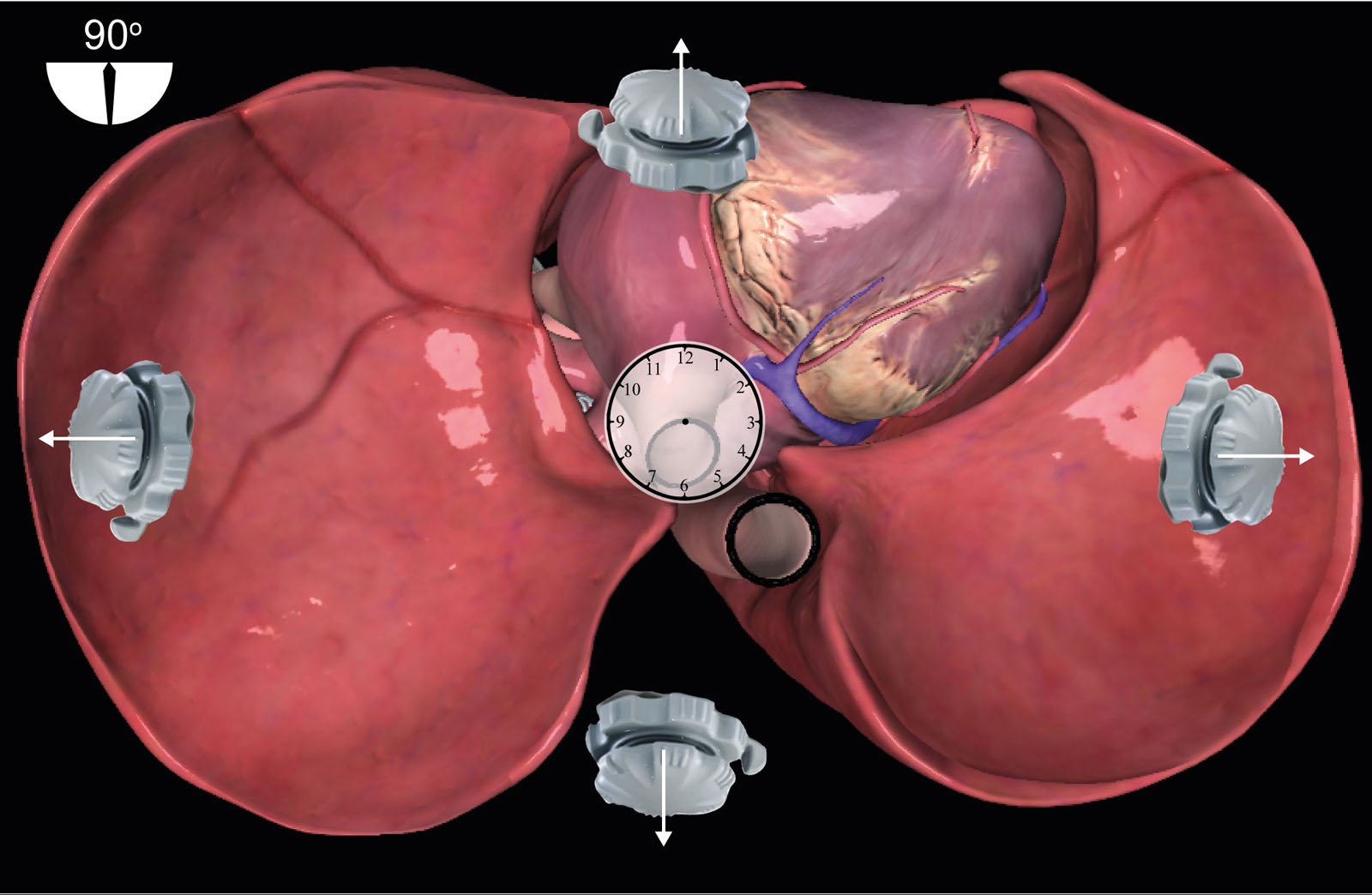
eFigure 32.4
TELUS TEE probe orientation. The US beam remains at 90°. The TEE knob represents a clock hand starting at 12 o’clock, then rotating counterclockwise from the left to 9, 6, 3 o’clock back to 12 o’clock. This allows the TEE knob position to identify the precise location of the US beam in the chest. Abbreviations: TEE, transesophageal echocardiography; TELUS, transesophageal lung ultrasound; US, ultrasound.
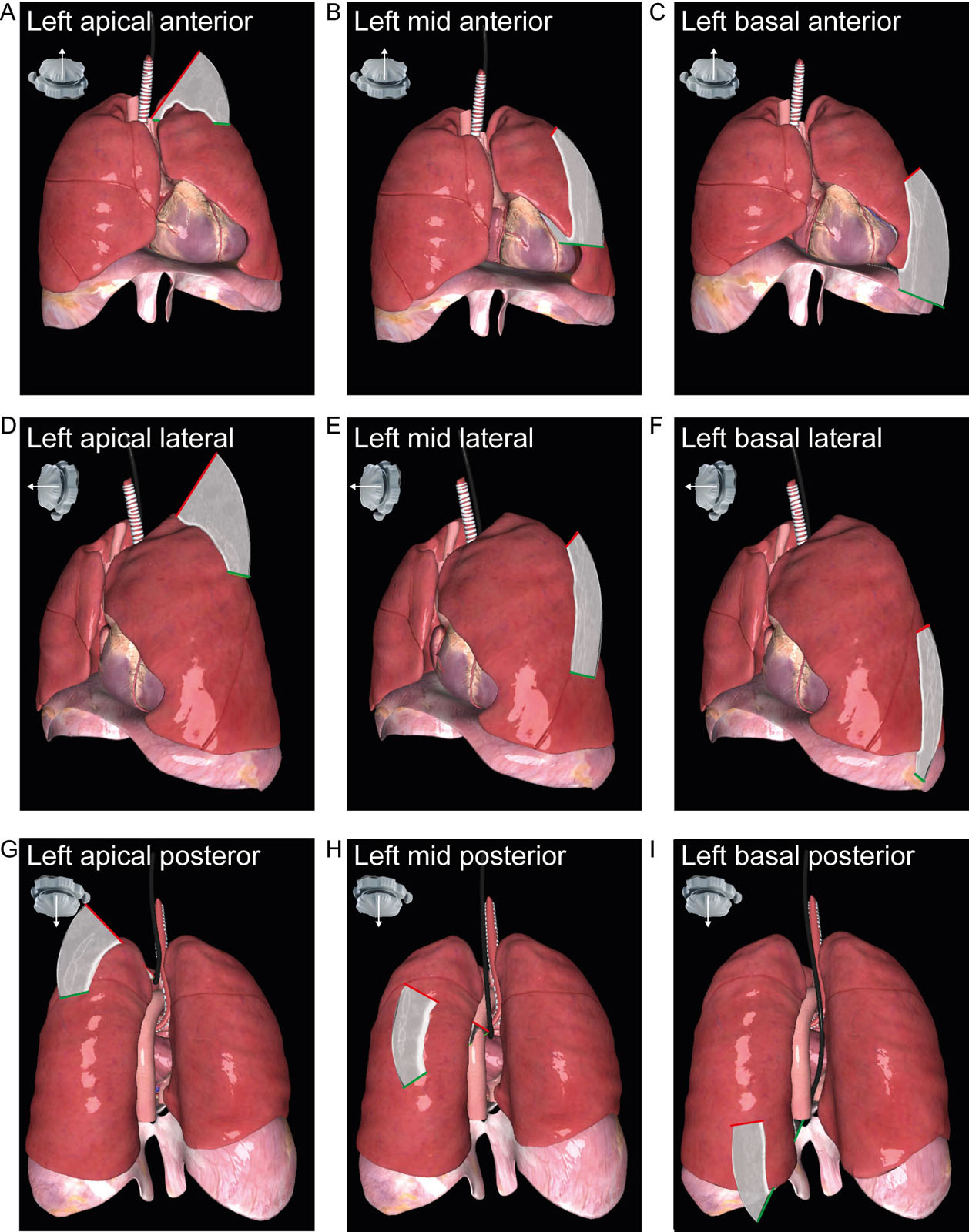
eFigure 32.5
TELUS examination. These diagrams represent TELUS examination of the left lung in the anterior region (A-C), lateral (D-F) and posterior (G-I) regions, as indicated by the yellow star. Abbreviations: TELUS, transesophageal lung ultrasound.
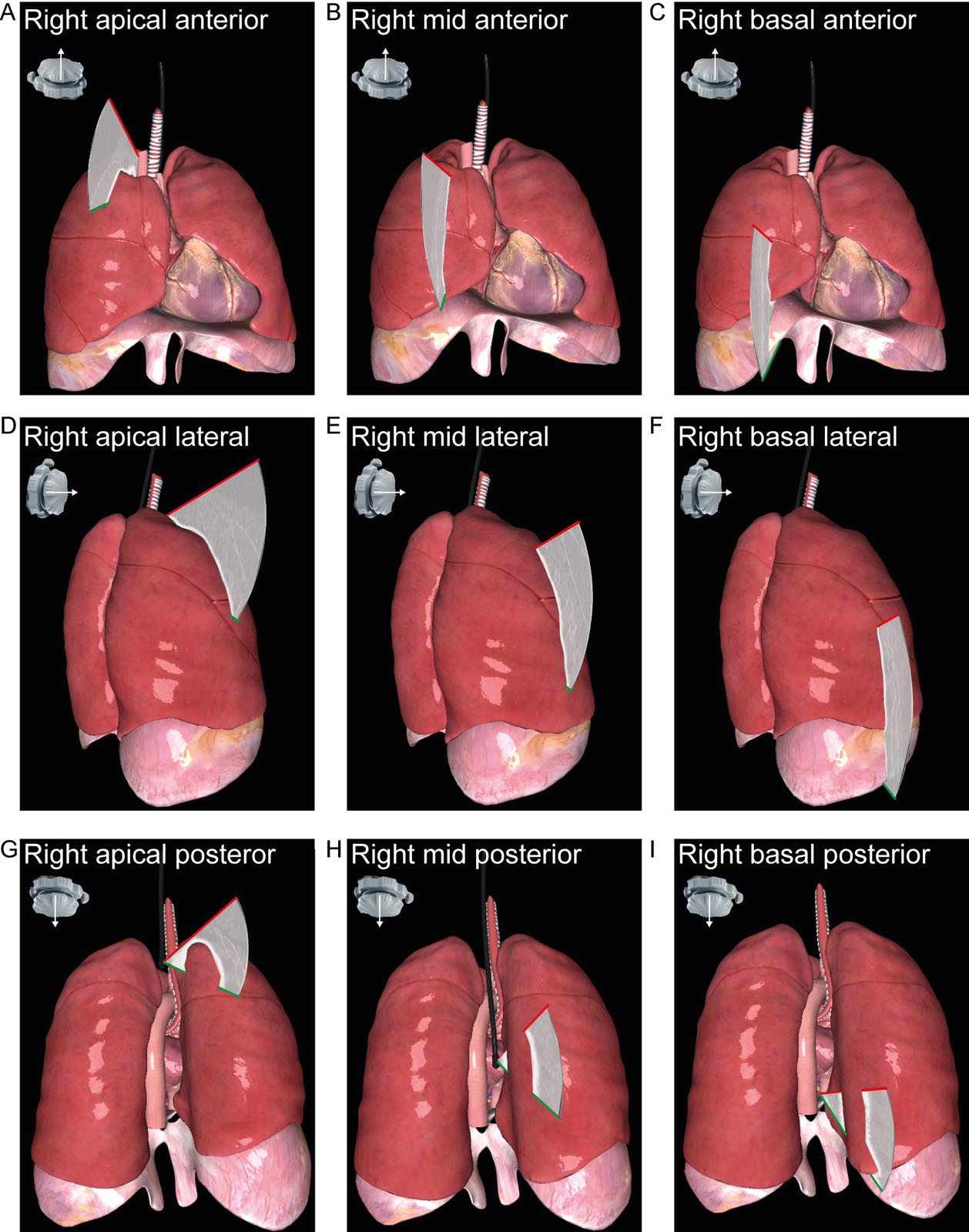
eFigure 32.6
TELUS examination. These diagrams represent TELUS examination of the right lung anterior region (A-C), lateral (D-F) and posterior (G-I) regions, as indicated by the yellow star. Abbreviations: TELUS, transesophageal lung ultrasound.
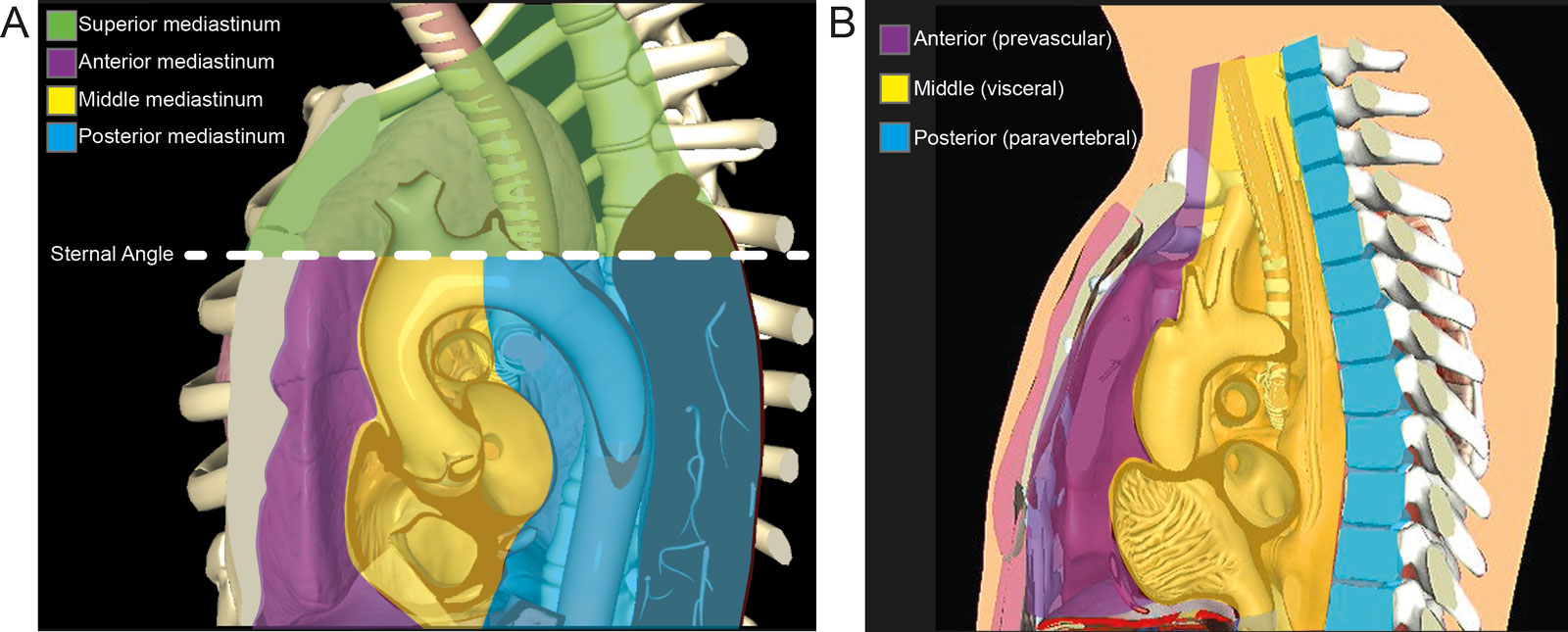
eFigure 32.13
Mediastinum anatomy. (A) This diagram shows the regions of the mediastinum as superior, anterior, middle, and posterior. The superior mediastinum is from the first rib to T4, the anterior mediastinum is from the sternum to the pericardium, the middle mediastinum is from T4 to T9, and the posterior mediastinum lies between the posterior pericardium to the spine. (B) More recent guidelines by the International Thymic Malignancy Interest Group divide the mediastinum in 3 regions.
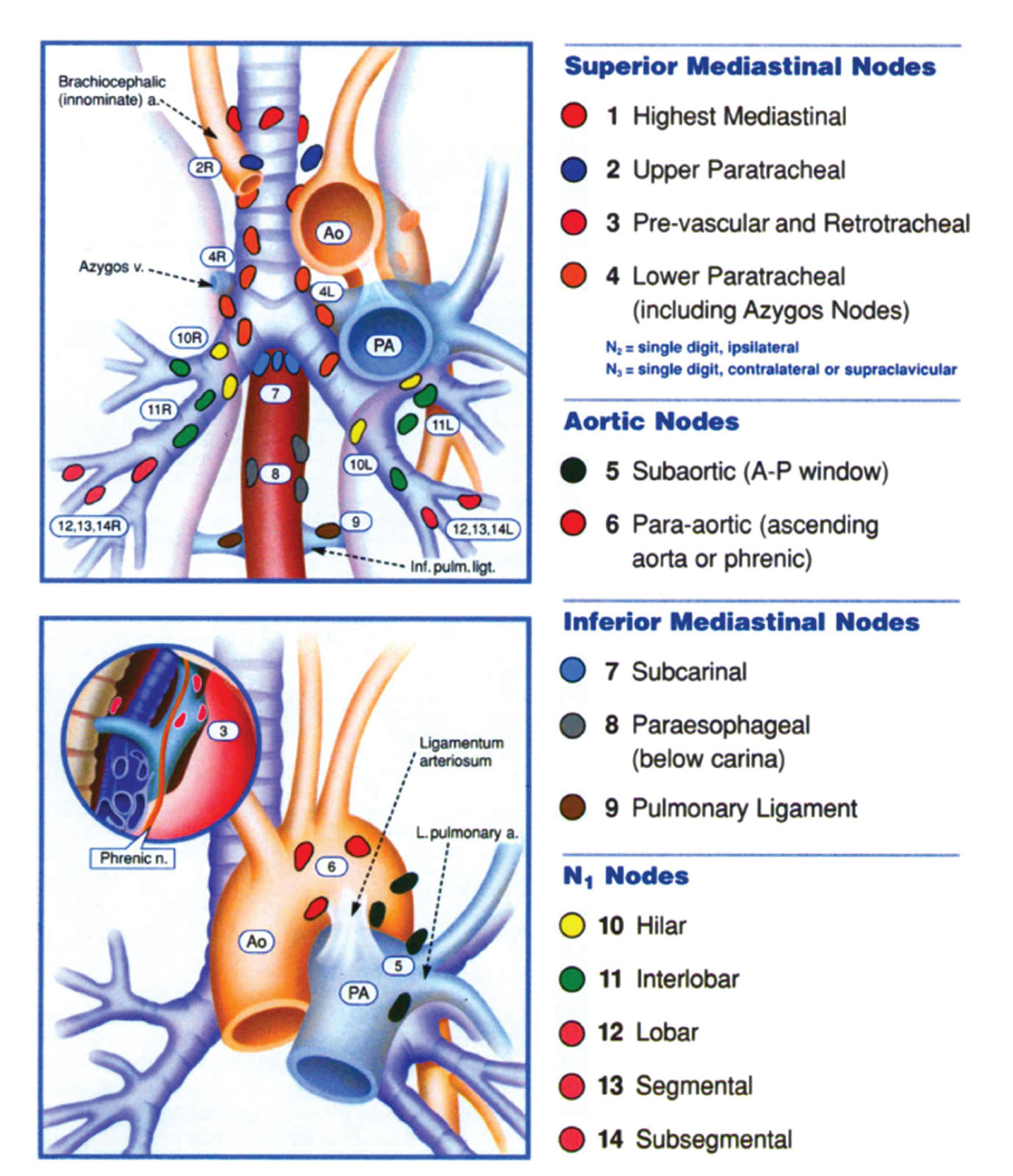
eFigure 32.14
Mediastinal lymph nodes. This is a diagram of the mediastinal lymph node stations for lung cancer staging. Abbreviations: a, artery; A, anterior; Ao aorta; inf, inferior; L, left; ligt, ligament; n, nerve; P, posterior; PA, pulmonary artery; pulm, pulmonary; v, vein. Source: With permission of Mountain CF et al.32
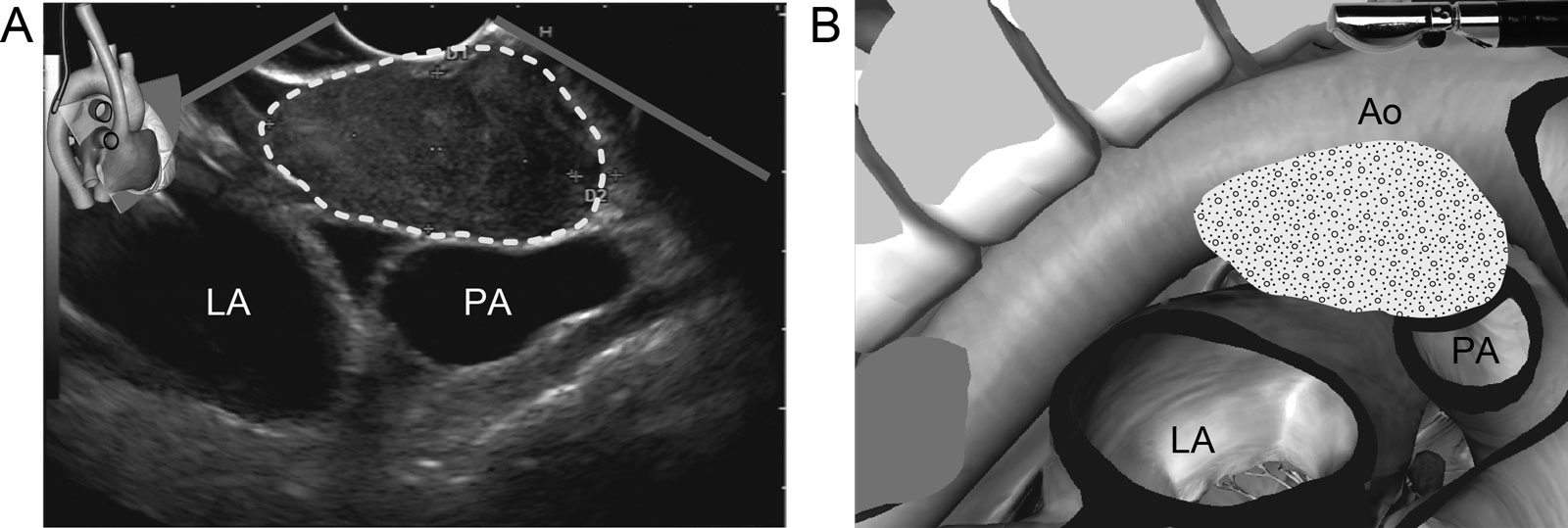
eFigure 32.15
Middle mediastinal pathology. (A,B) UE TEE view from endosonography of a malignant 4 X 2 cm sub-carinal lymph node (Station 7) in a patient with small-cell lung carcinoma. Abbreviations: Ao, aorta; LA, right atrium; PA, pulmonary artery; TEE, transesophageal echocardiography; UE, upper esophageal.
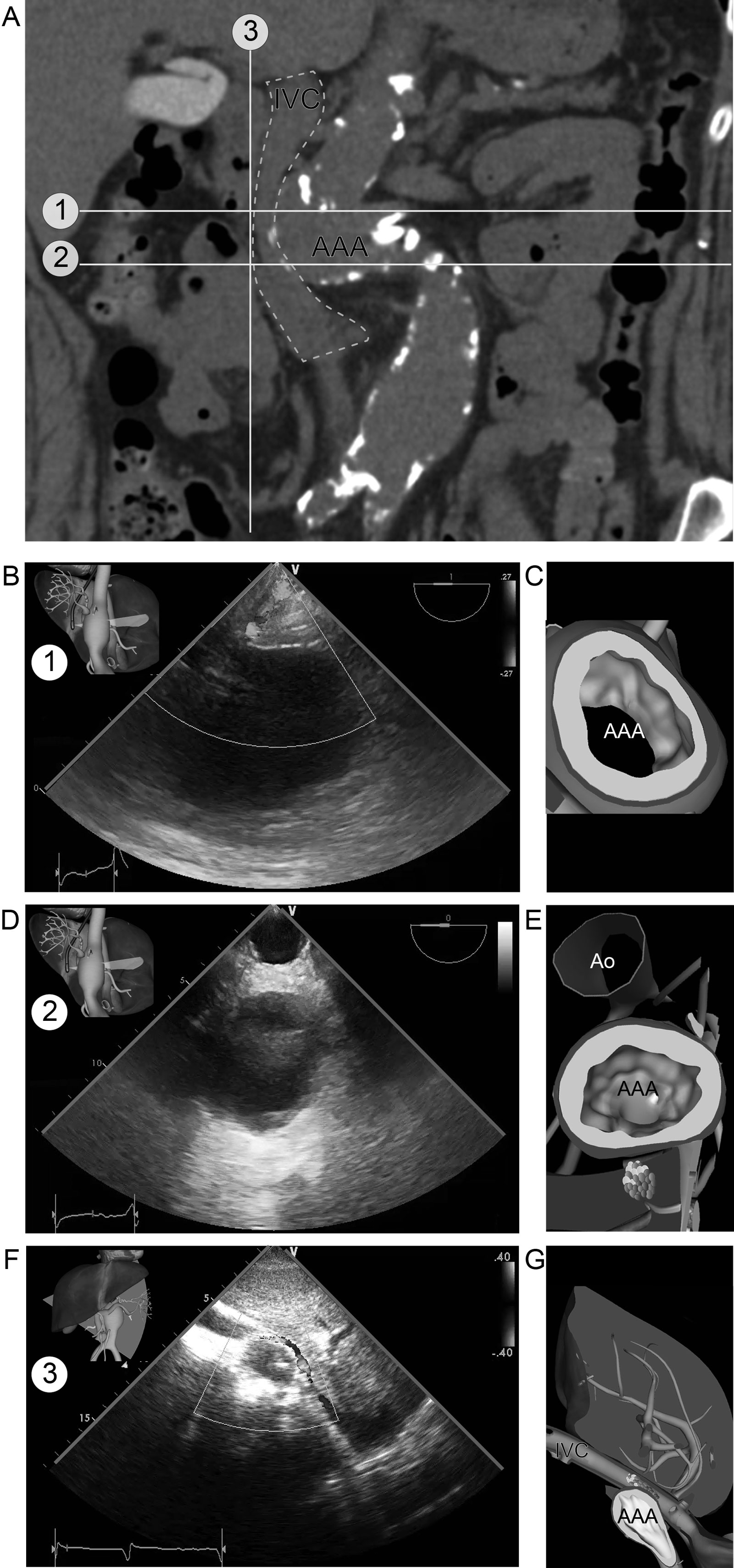
eFigure 32.24
Abdominal aortic aneurysm. This is a patient with an AAA compressing the IVC as seen by on (A) CT scan. Note the tortuous abdominal Ao. (B,C) Corresponding subcostal LAX view with IVC compression (plane #3 on CT scan) (D-G) TGAUS views. A cephalad view (plane #1 on CT scan) shows the AAA. A more caudal plane (plane #2 on CT scan) shows the AAA and the abdominal aorta on the same plane, giving the impression of 2 separate vessels. Abbreviations: AAA, abdominal aortic aneurysm; Ao, aorta; CT, computed tomography; IVC, inferior vena cava; LAX, long-axis; TGAUS, transgastric abdominal ultrasound.
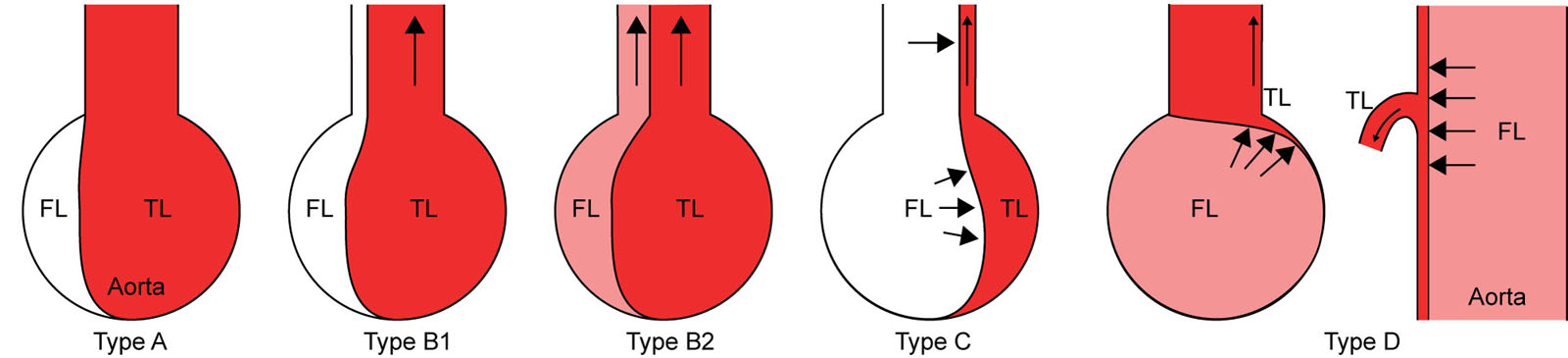
eFigure 32.26
Visceral artery perfusion. This schematic discloses the four perfusion patterns of visceral arteries. In Type A, there is no dissection in the branch artery with detectable blood flow. In Type B, the dissection extends into the branch artery with patent and dominant true lumen (TL) associated with small non-perfused (type B1) or perfused false lumen (FL) (type B2). Type C involves dissection extending into the branch artery with the narrowed TL compressed by FL without detectable blood flow. Type D has no dissection in the branch artery but the orifice obstructed by the intimal flap in the aorta. Clinically apparent intestinal ischemia was present in three cases: one case with Type C and two cases with Type D. Adapted from Orihashi et al.48
eFigure 32.34
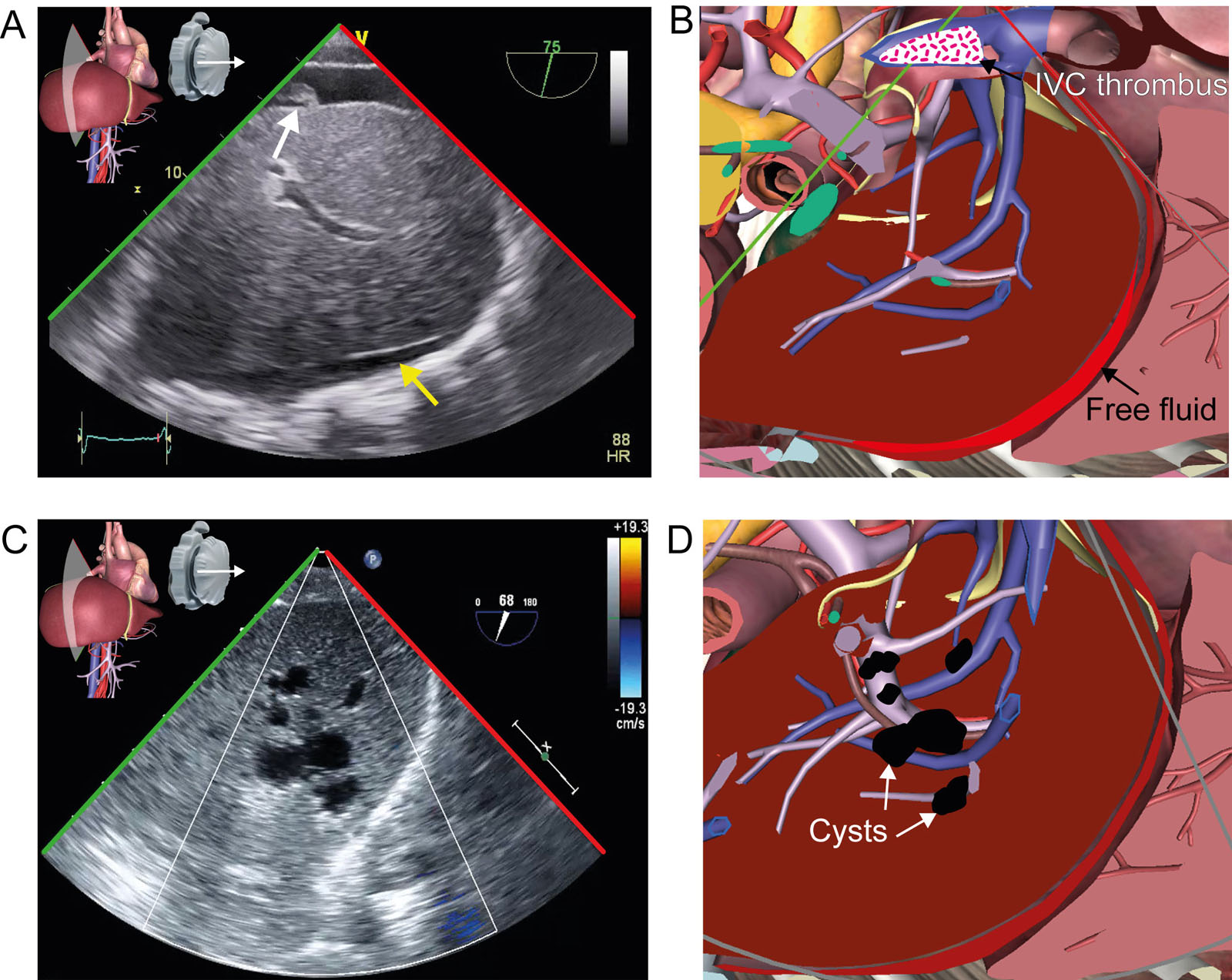
TGAUS IVC and liver view. (A,B) TGAUS IVC view after RVAD implantation shows an IVC thrombus (white arrow) and free abdominal fluid anterior to the liver (yellow arrow). (C,D) TGAUS view with CFI in a patient with multiple irregular liver cysts Abbreviations: CFI, color flow imaging; IVC, inferior vena cava; RVAD, right ventricular assist device; TGAUS, transgastric abdominal ultrasound. Adapted from Denault et al.4
eFigure 32.36
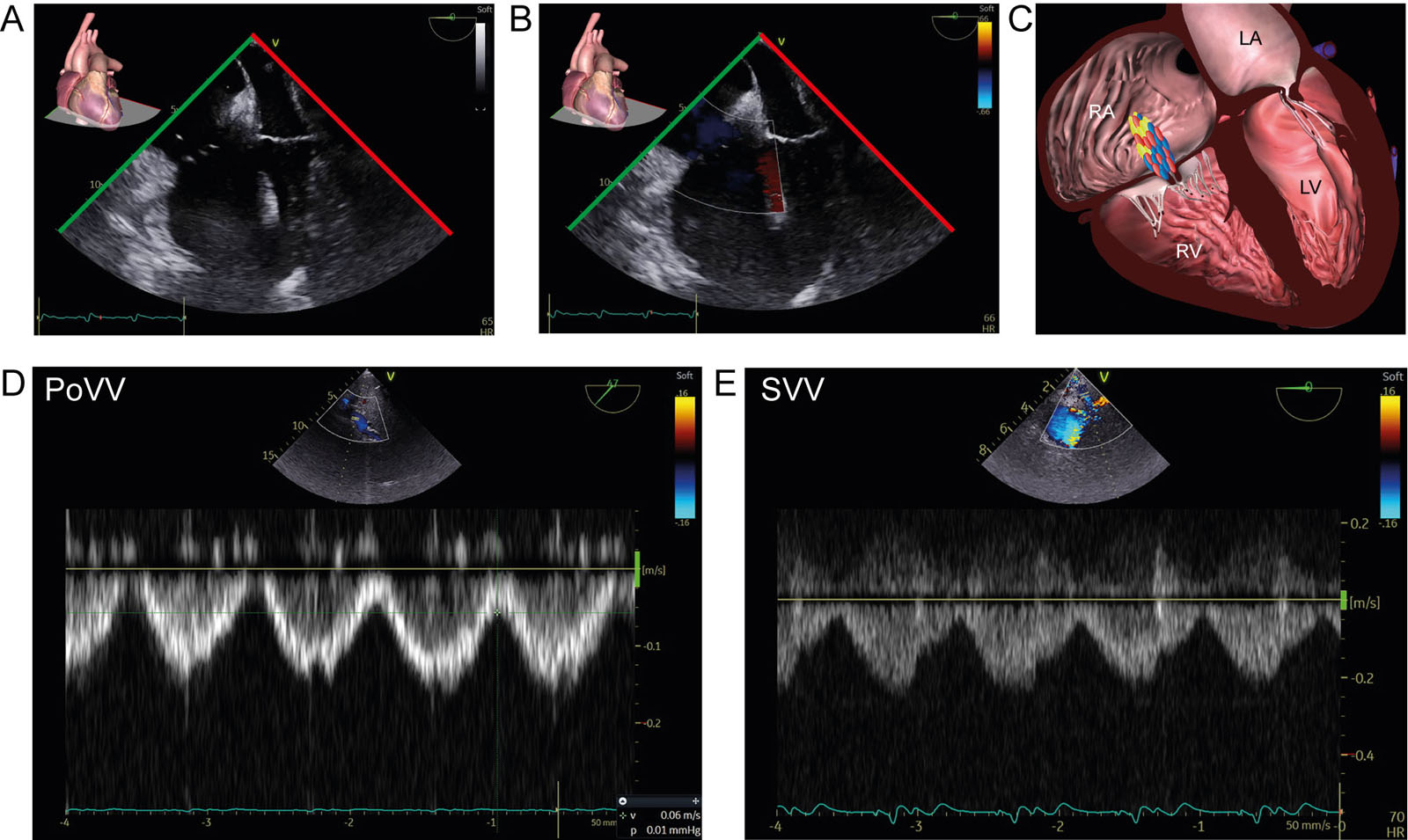
Splanchnic consequence of RV dysfunction. This is a 76-year-old man with cardiomyopathy admitted for lead-extraction. (A-C) ME 4C RV-focused views without and with CFI show RV dilatation without significant tricuspid regurgitation. (D,E) However, using TGAUS, there was significant portal and splenic vein pulsatility. The significant reduction in RA compliance will lead to pressure transmission during the cardiac cycle in the splanchnic and peripheral venous system without any significant tricuspid regurgitation. Abbreviations: 4C, four-chamber; CFI, color flow imaging; LA, left atrium; LV, left ventricle; ME, mid-esophageal; PoVV, portal vein velocity; RA, right atrium; RV, right ventricular; SVV, splenic vein velocity; TGAUS, transgastric abdominal ultrasound.
eFigure 32.42
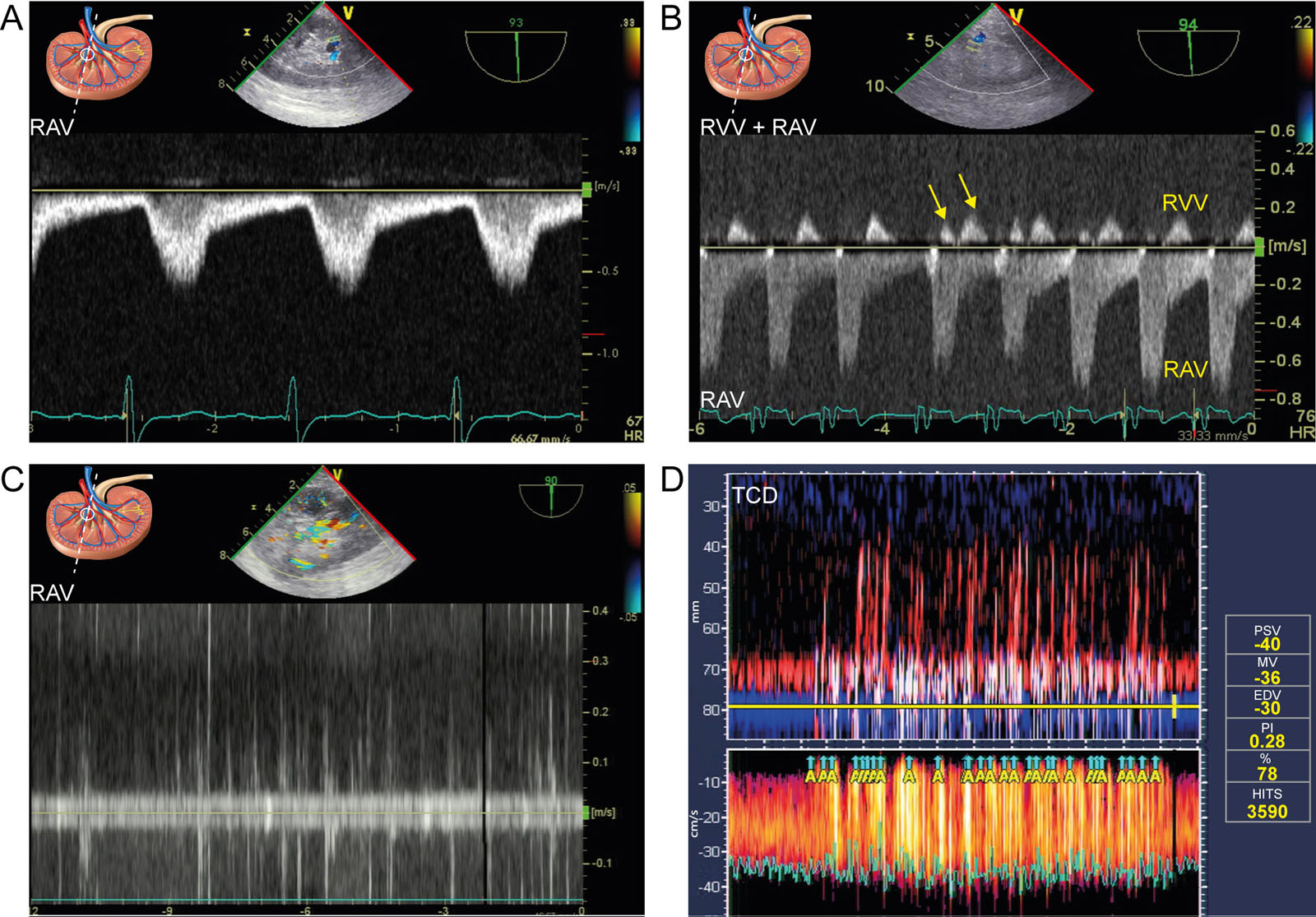
Renal Doppler abnormalities. (A) PWD of a RAV in a patient with aortic stenosis showing pulsus tardus or delayed peak systolic Doppler signal (arrow) and prolonged acceleration time (>70 msec). 86 (B) Abnormal RVV Doppler signal after CPB an uniphasic diastolic waveform and biphasic waveform on the fourth Doppler signal (arrows).93(C,D) Renal artery air embolism and simultaneous TCD upon unclamping at the end of CPB. Both monitoring techniques indicate emboli in multiple organs. A total of 3590 HITS occurred during the procedure, which correlates with increased morbidity and mortality.168 Abbreviations: CPB, cardiopulmonary bypass; EDV, end-diastolic velocity; HITS, high-intensity transient signals; MV, mean velocity; PI, pulsatility index; PSV, peak systolic velocity; PWD, pulsed-wave Doppler, RAV, renal artery velocity, RVV, renal vein velocity; TCD, transcranial Doppler. Adapted from Denault et al.4
eFigure 32.44
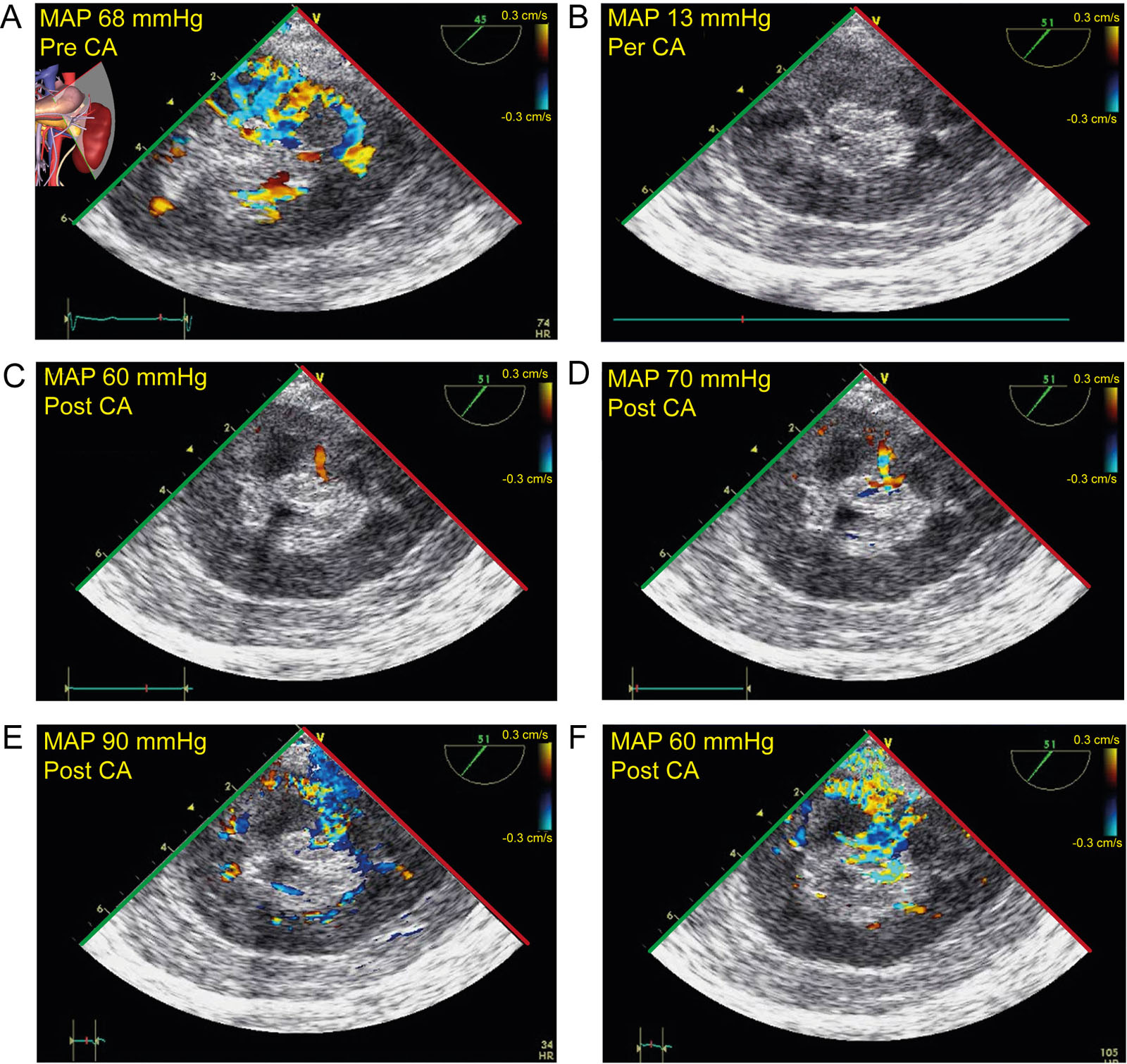
Renal CFI and arterial pressure. This is a 53-year-old man with coronary artery disease undergoing an aortic aneurysm repair. These are the TGAUS renal views with CFI at a very low velocity (A) before CA at a MAP 68 mmHg, (B) during CA at MAP 13 mmHg, there are no velocities but upon weaning from CPB, minimal CFI signals appear at (C) 60 mmHg, (D) 70 mmHg until the MAP reaches (E) 90 mmHg. Thereafter (F) a MAP of 60 mmHg had the same CFI signal as the baseline value. Abbreviations: CA, circulatory arrest; CFI, color flow imaging; CPB cardiopulmonary bypass; MAP, mean arterial pressure; TGAUS, transgastric abdominal ultrasound.
Videos
Chapter 32 Fig01
Chapter 32 Fig02AB
Chapter 32 Fig02CD
Chapter 32 Fig02EF
Chapter 32 Fig02GH
Chapter 32 Fig05ADG
Chapter 32 Fig06ADG
Chapter 32 Fig07A
Chapter 32 Fig07B
Chapter 32 Fig07C
Chapter 32 Fig07D
Chapter 32 Fig07E
Chapter 32 Fig07F
Chapter 32 Fig10A
Chapter 32 Fig10E
Chapter 32 Fig10F
Chapter 32 Fig11A
Chapter 32 Fig11B
Chapter 32 Fig12AC
Chapter 32 Fig15B
Chapter 32 Fig17
Chapter 32 Fig18A
Chapter 32 Fig18D
Chapter 32 Fig19A
Chapter 32 Fig19C
Chapter 32 Fig20A
Chapter 32 Fig20D
Chapter 32 Fig21_01
Chapter 32 Fig21_02
Chapter 32 Fig21_03
Chapter 32 Fig21_04
Chapter 32 Fig21_05
Chapter 32 Fig21_06
Chapter 32 Fig21_07
Chapter 32 Fig21_08
Chapter 32 Fig21_09
Chapter 32 Fig21_10
Chapter 32 Fig22A
Chapter 32 Fig23A
Chapter 32 Fig24A
Chapter 32 Fig24B
Chapter 32 Fig24D
Chapter 32 Fig24F
Chapter 32 Fig25A
Chapter 32 Fig25F
Chapter 32 Fig27A
Chapter 32 Fig28A
Chapter 32 Fig28B
Chapter 32 Fig28C
Chapter 32 Fig28D
Chapter 32 Fig28E
Chapter 32 Fig29A
Chapter 32 Fig29B
Chapter 32 Fig29C
Chapter 32 Fig29D
Chapter 32 Fig29E
Chapter 32 Fig29F
Chapter 32 Fig30A
Chapter 32 Fig30C
Chapter 32 Fig31A
Chapter 32 Fig31C
Chapter 32 Fig31D
Chapter 32 Fig31F
Chapter 32 Fig32F
Chapter 32 Fig33A
Chapter 32 Fig33B
Chapter 32 Fig33E
Chapter 32 Fig33G
Chapter 32 Fig34A
Chapter 32 Fig34C
Chapter 32 Fig35A
Chapter 32 Fig35E
Chapter 32 Fig36A
Chapter 32 Fig36B
Chapter 32 Fig37A
Chapter 32 Fig37D
Chapter 32 Fig37H
Chapter 32 Fig38A
Chapter 32 Fig38B
Chapter 32 Fig39A
Chapter 32 Fig39C
Chapter 32 Fig39E
Chapter 32 Fig40A
Chapter 32 Fig40D
Chapter 32 Fig41A
Chapter 32 Fig41C
Chapter 32 Fig41F
Chapter 32 Fig41H
Chapter 32 Fig41I
Chapter 32 Fig42C
Chapter 32 Fig42D
Chapter 32 Fig44A
Chapter 32 Fig45A
Chapter 32 Fig45D
Chapter 32 Fig46BC
Chapter 32 Fig46F
Tables
eTable 32.3 Ultrasound-guided differential diagnosis of acute hypoxemia
Diagnosis |
Lungs |
Left Heart |
Right Heart |
Pneumonia |
|
|
|
Obstructive atelectasis |
|
|
|
Massive pleural effusion |
|
|
|
ARDS |
|
|
|
Pneumothorax |
|
|
|
Pulmonary embolism |
|
|
|
LV failure |
|
|
|
Left valvular pathology |
|
|
|
Abbreviations: ARDS, acute respiratory distress syndrome; E/e’, ratio of the early transmitral filling (E) to the early mitral annular velocity (e’); IVC, inferior vena cava; LA, left atrium; LAX, long-axis; LV, left ventricle; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; PH, pulmonary hypertension; RA, right atrium; RV, right ventricle; RVEF, right ventricular ejection fraction; RVOT, right ventricular outflow tract; SAM, systolic anterior motion; SPAP, systolic pulmonary artery pressure. (With permission of Cavayas et al.3) |
|||
eTable 32.5 Clinical role of TGAUS views in the operating room and intensive care unit
| TGAUS Views | Clinical Role |
| Celiac trunk view #1 and SMA-renal confluence view #2 | Vascular monitoring during aortic dissection and vascular stenting;42, 119,37,45,120,121, 48,43,40 [DB1] detection of compromised splanchnic flow with celiac trunk and mesenteric artery monitoring,48 splanchnic vascular stenosis,49 nutcracker syndrome122, intra-aortic balloon pump positioning39 |
| Stomach view #3 | Full stomach, upper gastrointestinal bleeding, gastric varices, free peritoneal fluid.35,119 |
| Inferior vena cava and hepatic veins views #4 | Diagnosis of RV systolic and diastolic dysfunction,123-126,83, 71, 127, 66, 128 pulmonary hypertension,129-131 assessment for IVC stenosis in liver transplantation, heart transplantation, ECMO and artificial heart,132, 133, 73, 134, 71, 72, 135, 136, 37, 137, 24 ruling-out abdominal IVC tumor138, 57, 139-142, 61, 105, 108, 143, 65, 144, 145, 104, 146 or thrombus147, 140, 141, 148, 64, 143, 149, 74 as a cause of pulmonary embolism and right-to-left shunting through a PFO in hypoxic patients with right heart dilatation,147, 140, 141, 148, 64, 143, 149 abdominal compartment syndrome;150, 71, 24 intraoperative monitoring during renal cell carcinoma surgery involving the inferior vena cava.57, 151-154, 105, 107, 155, 108, 143, 65, 156, 144, 145, 102, 104, 157, 106, 146, 109 |
| Portal triad view #5 | Abdominal compartment syndrome,35, 150, 71 mesenteric ischemia with portal venous air,35, 48 hepatic artery and portal vein stenosis in liver transplantation,134, 74 portal venous Doppler monitoring right ventricular dysfunction associated with venous congestion,92, 119, 76, 60 evaluation of response to medical treatment.92, 123 |
| Liver view #6 | Detection of cirrhosis and ascites,119, 61 liver abscess or cysts,119 transjugular portal systemic shunt,75 liver transplantation and resection.158, 75, 74, 159 |
| Spleen view #7 | Free abdominal fluid and splenic rupture in trauma,35, 87 splenic venous Doppler monitoring right ventricular dysfunction associated with venous congestion,92, 119, 76, 60 evaluation of response to medical treatment,92, 123 |
| Kidney view #8 | Oligoanuria: renal arterial hypoperfusion or elevate renal resistance index,98, 160, 88, 51, 90, 161, 162, 46, 89, 91 renal venous congestion92, 89 left hydronephrosis and renal artery air embolization92 and differentiating acute versus chronic renal failure.119 |
| Pancreatic view #9 and sub-pancreatic splenic vessels view #10 | Splenic venous Doppler monitoring right ventricular dysfunction associated with venous congestion 76 92,119,60 and evaluation of response to medical treatment.92, 123 |
| Abbreviations: ECMO, extra-corporeal membrane oxygenation; IVC, inferior vena cava; PFO, patent foramen ovale; RV, right ventricular; SMA, superior mesenteric artery; TGAUS, transgastric abdominal ultrasound. | |