Figures
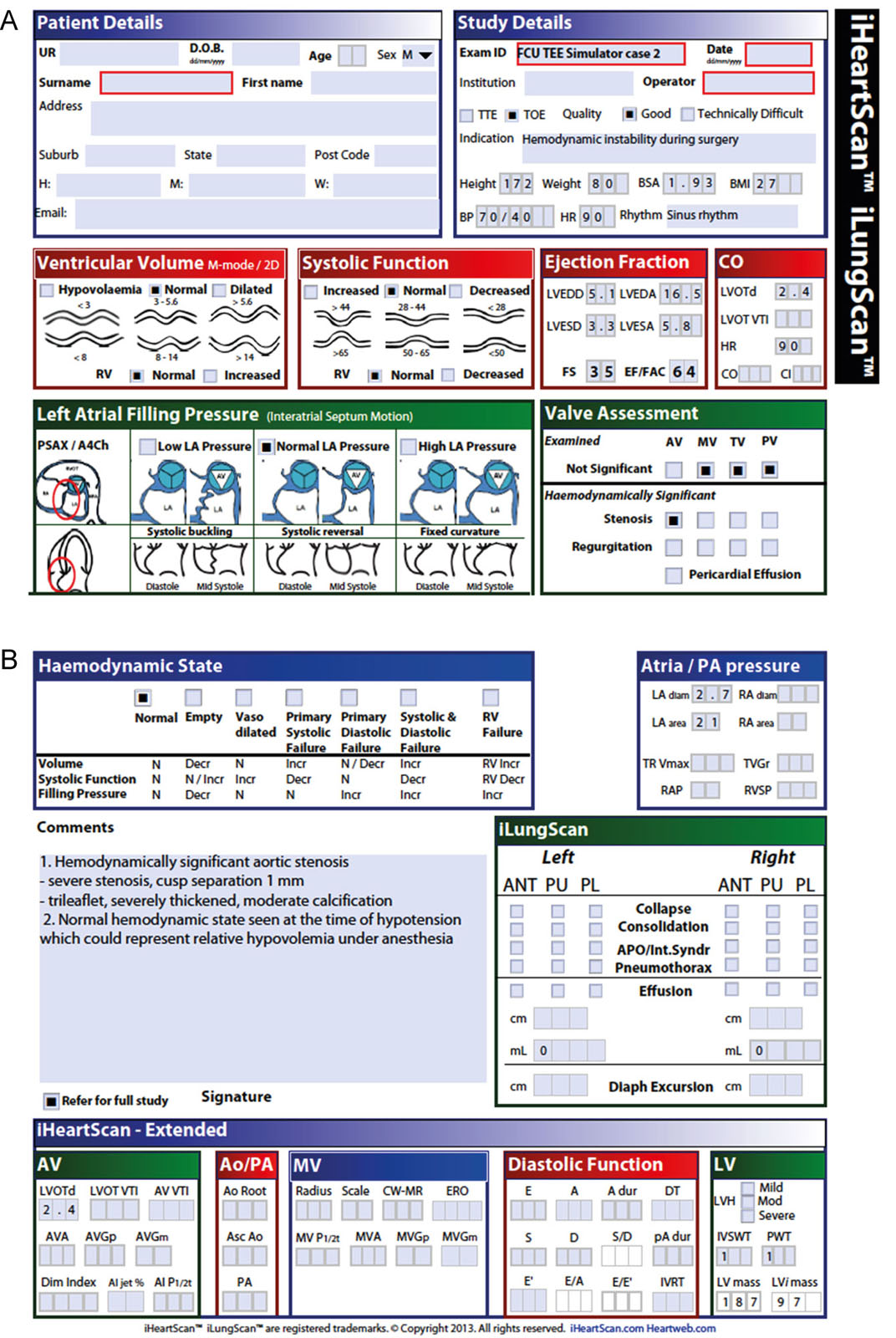
eFigure 34.12
iTeachU Focused Cardiac Ultrasound TEE and TTE course. (A,B) Format of the interpretive report which includes the patients and study details, assessment of ventricular function, filling pressure, valves, hemodynamic state, lung scanning and extended iHeartScan. Courtesy of iEachU David Canty, Melbourne University, Australia.
Videos
Chapter 34 Fig03B
Chapter 34 Fig03E
Chapter 34 Fig03F
Chapter 34 Fig04A
Chapter 34 Fig06
Chapter 34 Fig07A
Chapter 34 Fig07C
Chapter 34 Fig07D
Chapter 34 Fig08CD
Chapter 34 Fig10A
Chapter 34 Fig10B
Chapter 34 Fig11
Chapter 34 Fig13
Chapter 34 Fig14
Chapter 34 Fig15A
Chapter 34 Fig15B
Tables
eTable 34.1 ASA and SCVA 2010 recommendations for using perioperative TEE
Cardiac and Thoracic Aortic Procedures |
|
|
|
|
Noncardiac Surgery |
|
Critical Care |
|
Abbreviations: ASA, American Society of Echocardiography; CABG, coronary artery bypass graft; SCVA, Society of Cardiovascular Anesthesia; TEE, transesophageal echocardiography. Adapted from 7 |
eTable 34.3 Recommended training objectives for basic and advanced perioperative TEE
Basic Training |
Cognitive Skills (Knowledge of) |
|
Technical Skills (Ability to) |
|
Advanced Training |
Cognitive Skills (Knowledge of) |
|
Cognitive Skills |
Technical Skills (Ability to) |
|
Modified from the American Society of Echocardiography and Society of Cardiovascular Anesthesiologists Task Force Guidelines for Training in Perioperative Echocardiography 2002. 12 |
eTable 34.4 Echocardiography training guidelines
| Guidelines | Basic | Advanced | Director | |||||||
| Total Exams | TEE Exams | Total Exams | TEE Exams | Total Exams | TEE Exams | |||||
| American Society of Echocardiography and Society of Cardiovascular Anesthesiology guidelines for training in perioperative echocardiography (2002 and 2006) | ||||||||||
| Number of studies | 150 | 50 performed | 300 | 150 performed | 450 | 300 | ||||
| Training duration | Not specified | Not specified | Not specified | |||||||
| Total CME hours | 20 | 50 | Not specified | |||||||
| MOC: CME hours | 15 within 3 years | 15 within 3 years | 15 within 3 years | |||||||
| MOC: # TEE/ year | 50 interpreted 25 performed | 50 interpreted 25 performed | 50 interpreted 25 performed | |||||||
| American College of Cardiology/American Heart Association guidelines for training in TTE and TEE (2003) and COCATS 3 (2008) | ||||||||||
| Number of studies | 150 interpreted; 75 performed | 300 interpreted150 performed | 750 interpreted 300 performed | Not specified | ||||||
| Training duration (months) | 3 | 6 | 12 | |||||||
| Total CME hours | Not specified | Not specified | Not specified | |||||||
| MOC: CME hours | 5 | 5 | >5 | |||||||
| MOC: # TEE/ year | NA | 20-50 | Not specifies | |||||||
| Canadian Anesthesiologists’ Society and Canadian Society of Echocardiography (2006 and 2023) | ||||||||||
| Number of studies | 150 | 100 performed | 300 | 200 performed | 450 | 300 | ||||
| Training duration (months) | 3 | 6 | 9 | |||||||
| Total CME hours | 50 within 2 years | 50 within 2 years | 75 within 2 years | |||||||
| MOC: CME hours | 50 within 4 years | 50 within 4 years | 75 within 4 years | |||||||
| MOC: # TEE/year | 50 | 50 | 50 (75) | |||||||
| European Society of Echocardiography (2010) | ||||||||||
| Number of studies | 250/150 | 75/125 | NS | NS | ||||||
| MOC: CME hours | 30 within 5 years | 30 within 5 years | 30 within 5 years | |||||||
| MOC: # TEE/year | 50 | 50 | 50 | |||||||
| Abbreviations: CME, continuing medical education; MOC, maintenance of certification; NA, not applicable; NS, not specified; NS: not specified; TEE, transesophageal echocardiography; TTE, transthoracic echocardiography. Adapted from Hahn et al. 12 | ||||||||||
eTable 34.5 Intraoperative echocardiography report
Basic components of an intra-operative transesophageal echo report should include the following basic demographics. The content of the report should address the indications for the study and may include some or all of the following components. |
|||
|
|
||
Reporting the following structures as normal implies a complete examination. |
|||
|
|||
|
|
|
|
The study should incorporate a final assessment of the patient based on the intra-operative findings and include the following. |
|||
|
|||
The above constitutes a basic examination. Specific indications or pathology require further targeted imaging and/or hemodynamic assessment. Abbreviations: CABG, coronary artery bypass grafting; ER, emergency room; ICU, intensive care unit; OR, operating room; PACU, postoperative anesthesia care unit; TTE, transthoracic echocardiography. Reproduced from the Canadian guidelines for training in adult perioperative transesophageal echocardiography.19 |
|||