Figures
eFigure 9.13
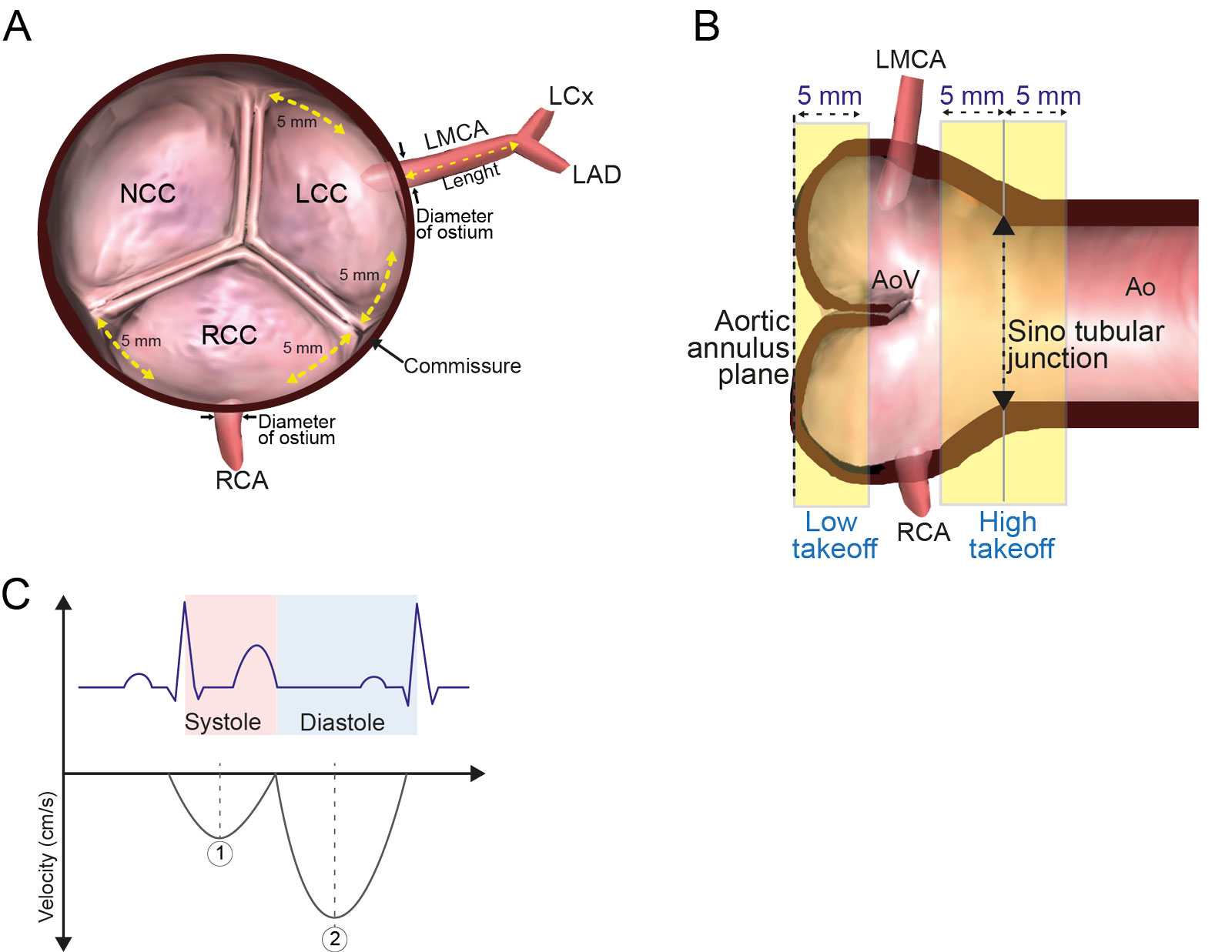
Coronary artery measurements. These schematic diagrams show the TEE findings and measurement criteria for coronary arteries. (A) Diagram of the ME AoV SAX view shows the location of anomalous origin and measurements of the LMCA length and the LMCA and RCA ostial diameters. The coronary origin was defined as anomalous if it was located within 5 mm of the commissure in the ME AoV SAX view. (B) Diagram of the ME AoV LAX view illustrating low and high orifice takeoff relative to the aortic annulus and STJ. Low takeoff was defined as within 5 mm from the annulus, whereas high takeoff was defined as within 5 mm below or above the STJ. (C) Schematic of normal coronary flow spectral envelope presenting as a continuous flow with diastolic predominance relative to the ECG and cardiac cycle. Abbreviations: Ao, aorta; AoV, aortic valve; ECG, electrocardiographic; LAD, left anterior descending artery; LAX, long-axis; LCC, left coronary cusp; LCx, left circumflex artery; LMCA, left main coronary artery; ME, mid-esophageal; NCC, non-coronary cusp; RCA, right coronary artery; RCC, right coronary cusp; SAX, short-axis; STJ, sinotubular junction; TEE, transesophageal echocardiography. Modified from Kasprzak 59 and Kondo et al. 57 and Kasprzak et al.
eFigure 9.15
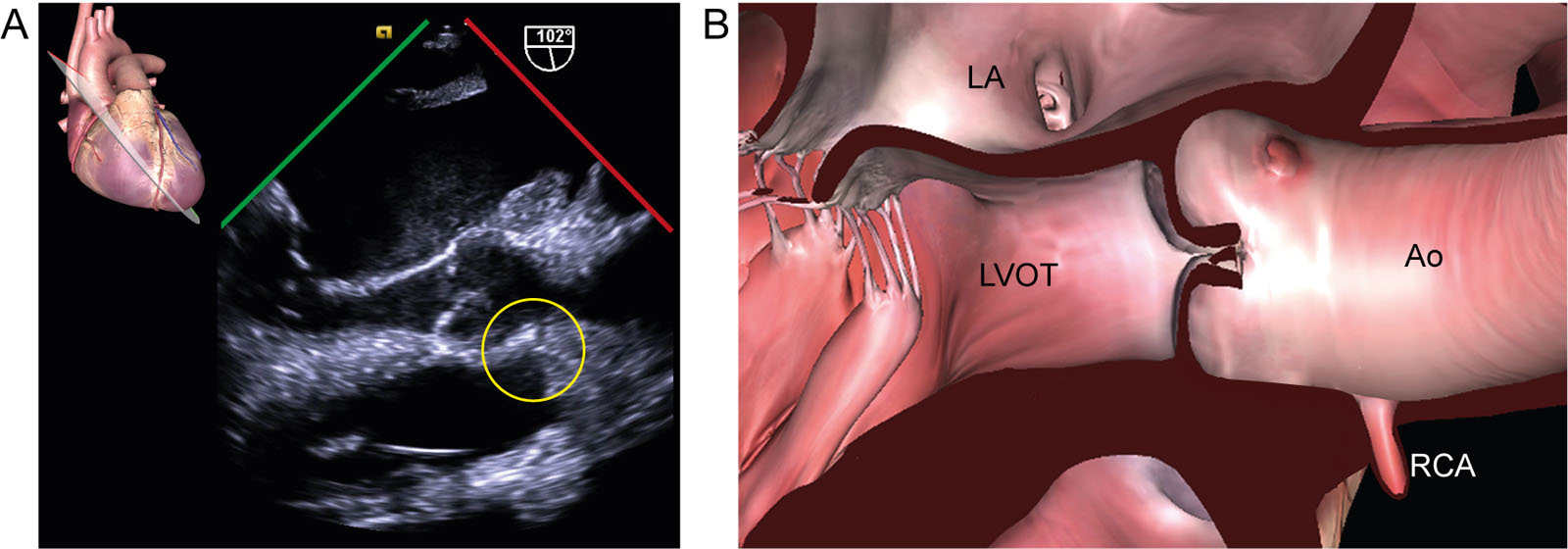
Anomalous coronary artery. (A, B) ME AoV LAX view from a 73-year-old female patient with rheumatic mitral stenosis without known congenital anomalies or connective tissue disease. There is an abnormal origin of the RCA above the STJ (yellow circle). In such cases, the surgeon needs to use caution to avoid coronary steal while de-airing through the Ao-root vent and coronary obstruction (or kinking) by pledget reinforcement sutures. Abbreviations: Ao, aorta; AoV, aortic valve; LA, left atrium; LAX, long-axis; LVOT, left ventricular outflow tract; ME, mid-esophageal; RCA, right coronary artery; STJ, sinotubular junction.
eFigure 9.17
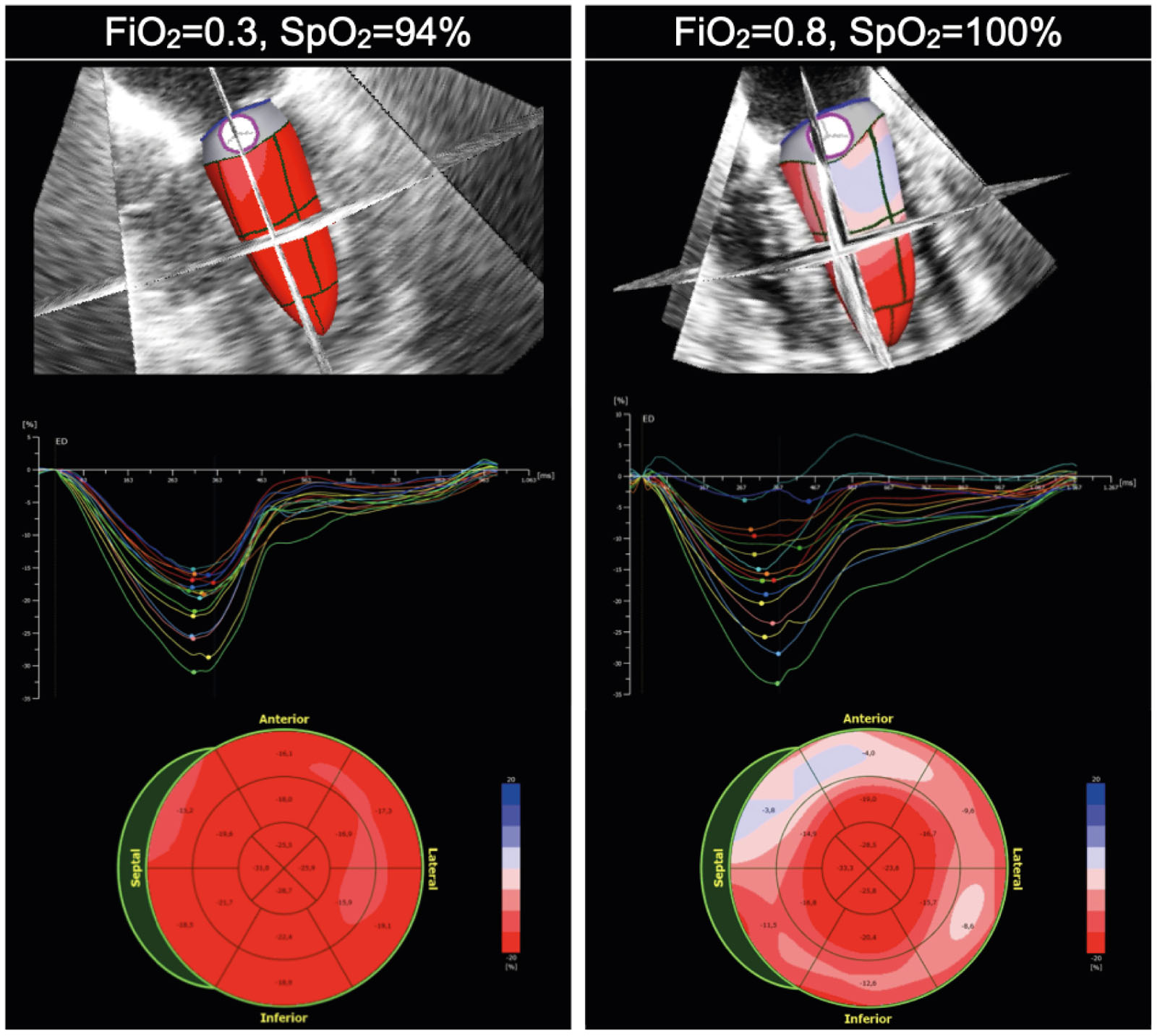
Strain in hyperoxia. In patients with normal contractile function, hyperoxia may be associated with a decrease in systolic function and changes in regional wall motion, as seen in these strain curves and bull’s eyes when increasing the FiO2 from 30% to 80%. Abbreviations: FiO2, inspired oxygen concentration; SpO2, oxygen saturation using pulse oximetry.
eFigure 9.19
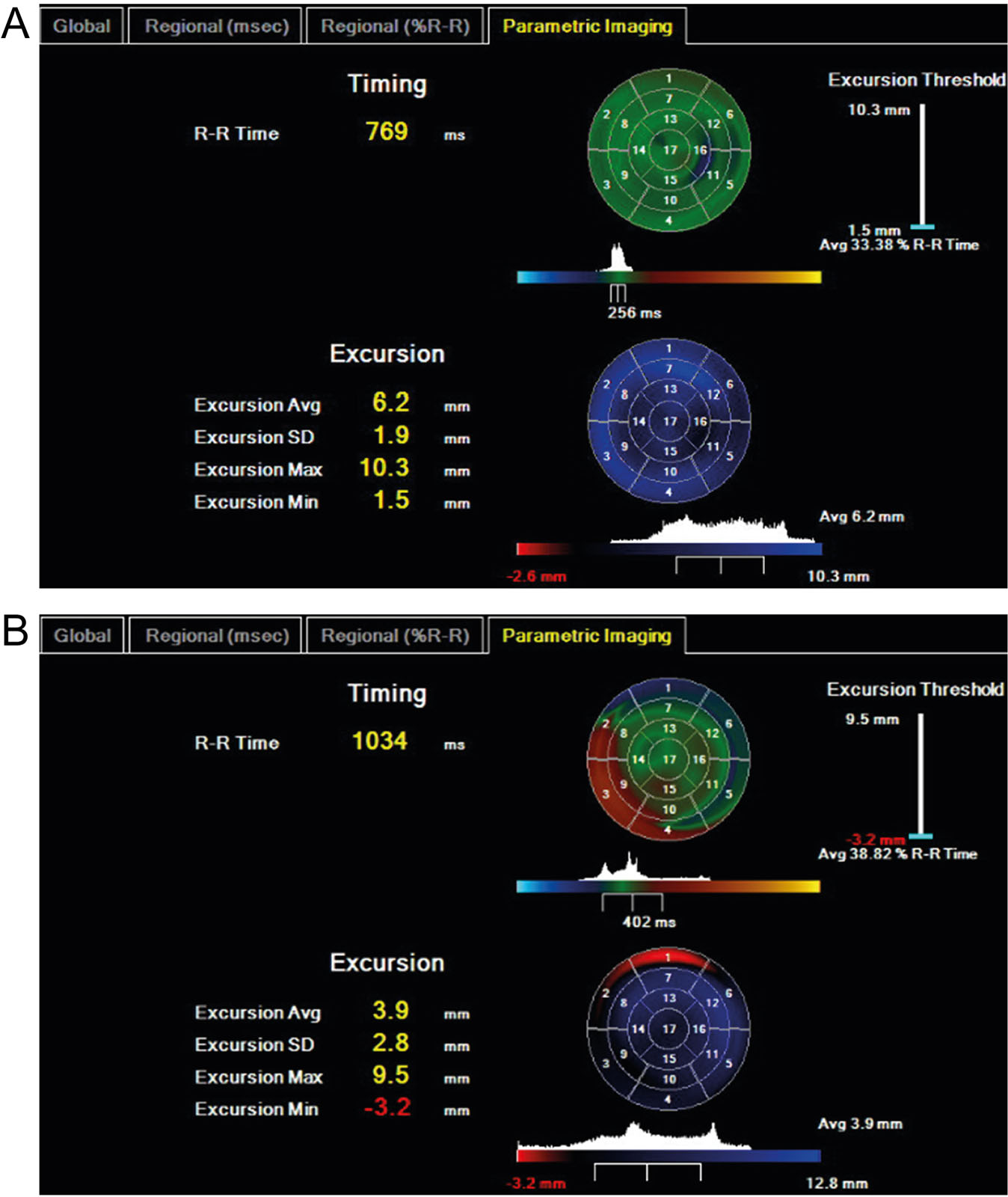
LV timing and excursion. Real time three-dimensional echocardiography analysis showing (A) normal and (B) abnormal bull’s-eye parametric displays of regional timing and excursion in a TTE orientation. For timing, the green color indicates average timing, blue color, early contraction and red color, delayed contractions. For excursion, the blue color indicates normal inward motion; black color is an akinetic segment and red is dyskinetic segments. Abbreviations: Avg, average; LV, left ventricle; SD, standard deviation; TTE, transthoracic echocardiography. . Adapted from Aggarwal et al.33
eFigure 9.28
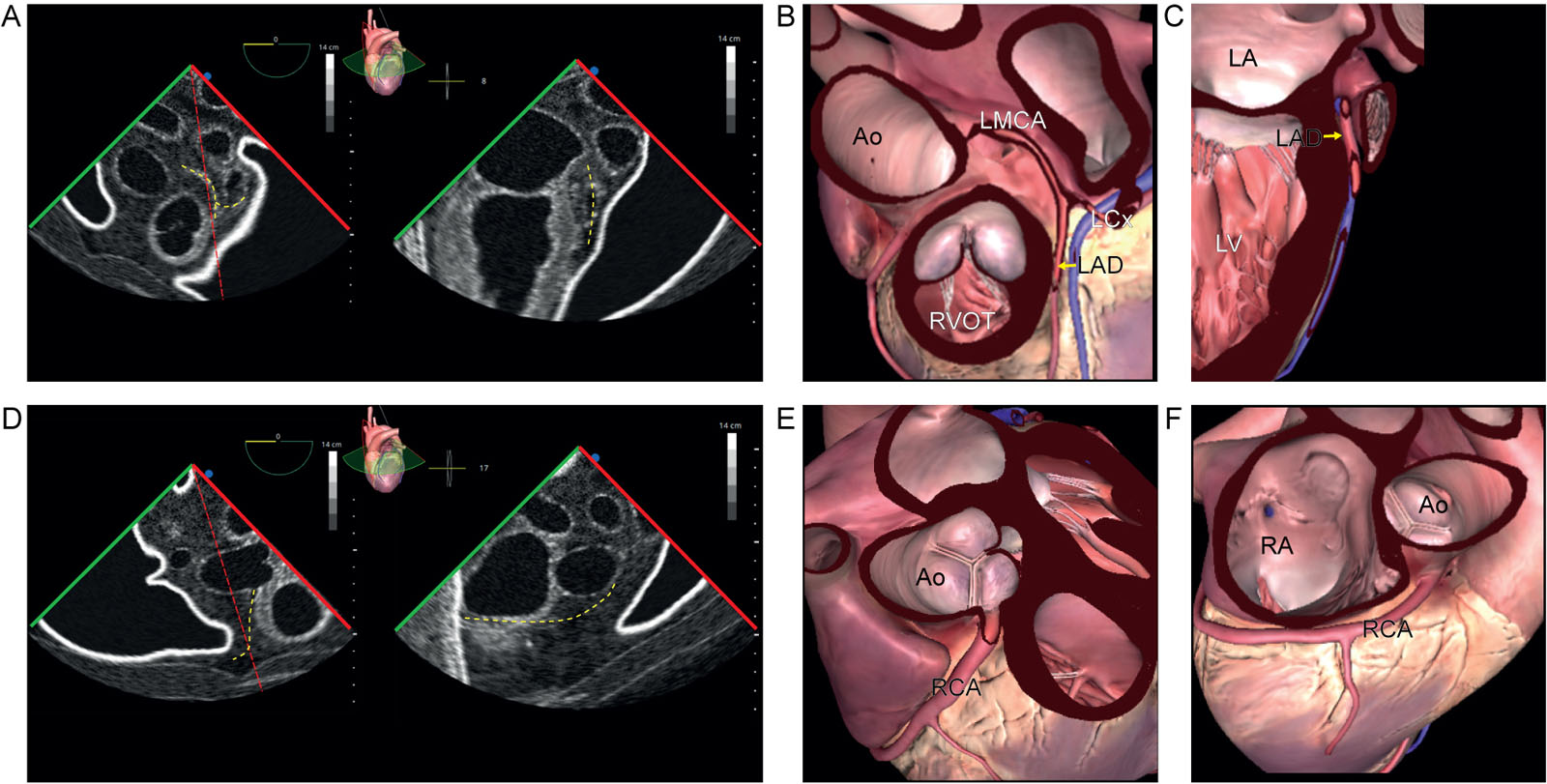
Biplane coronary views 0° and 90°. (A-H) ME biplane views and diagrams at 0° and 90° using a TEE simulator with a focus on the (A-D) LCA and (E-H) RCA. Abbreviations: Ao, aorta; LA, left atrium; LAD, left anterior descending; LCA, left coronary artery; LCx left circumflex artery; LMCA, left main coronary artery; LV, left ventricle; ME, mid-esophageal; RA, right atrium; RCA, right coronary artery; RVOT, right ventricular outflow tract; TEE, transesophageal echocardiography.
eFigure 9.29
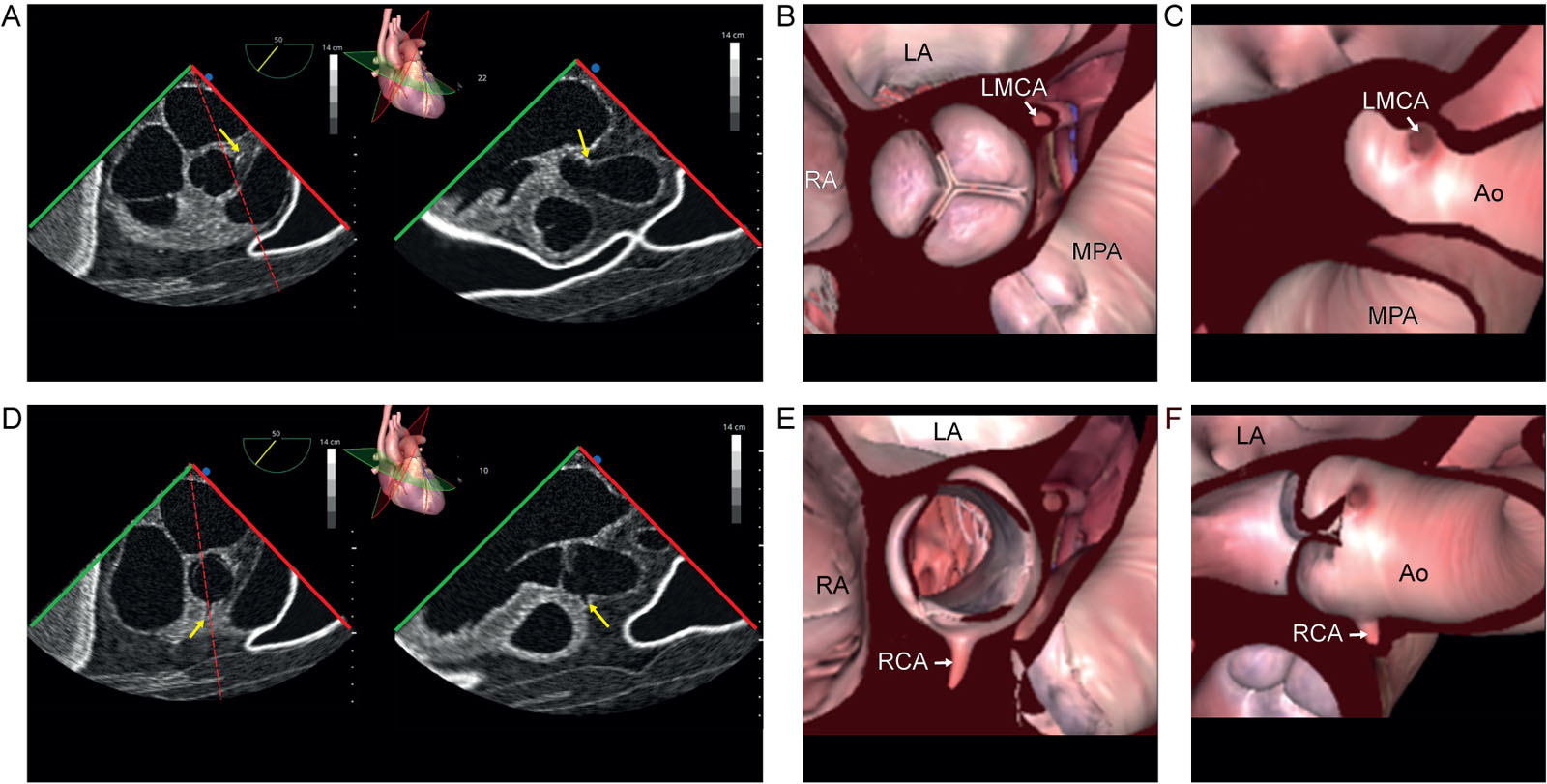
Biplane coronary views 50° and 140°. (A-H) ME biplane views and diagrams at 50° in SAX and 140° in LAX using a TEE simulator with a focus on the origins of the (A-D) LCA and (E-H) RCA. Abbreviations: Ao, aorta; LA, left atrium; LAX, long-axis; LCA, left coronary artery; LMCA, left main coronary artery; ME, mid-esophageal; MPA, main pulmonary artery; RA, right atrium; RCA, right coronary artery; SAX, short-axis; TEE, transesophageal echocardiography.
eFigure 9.30
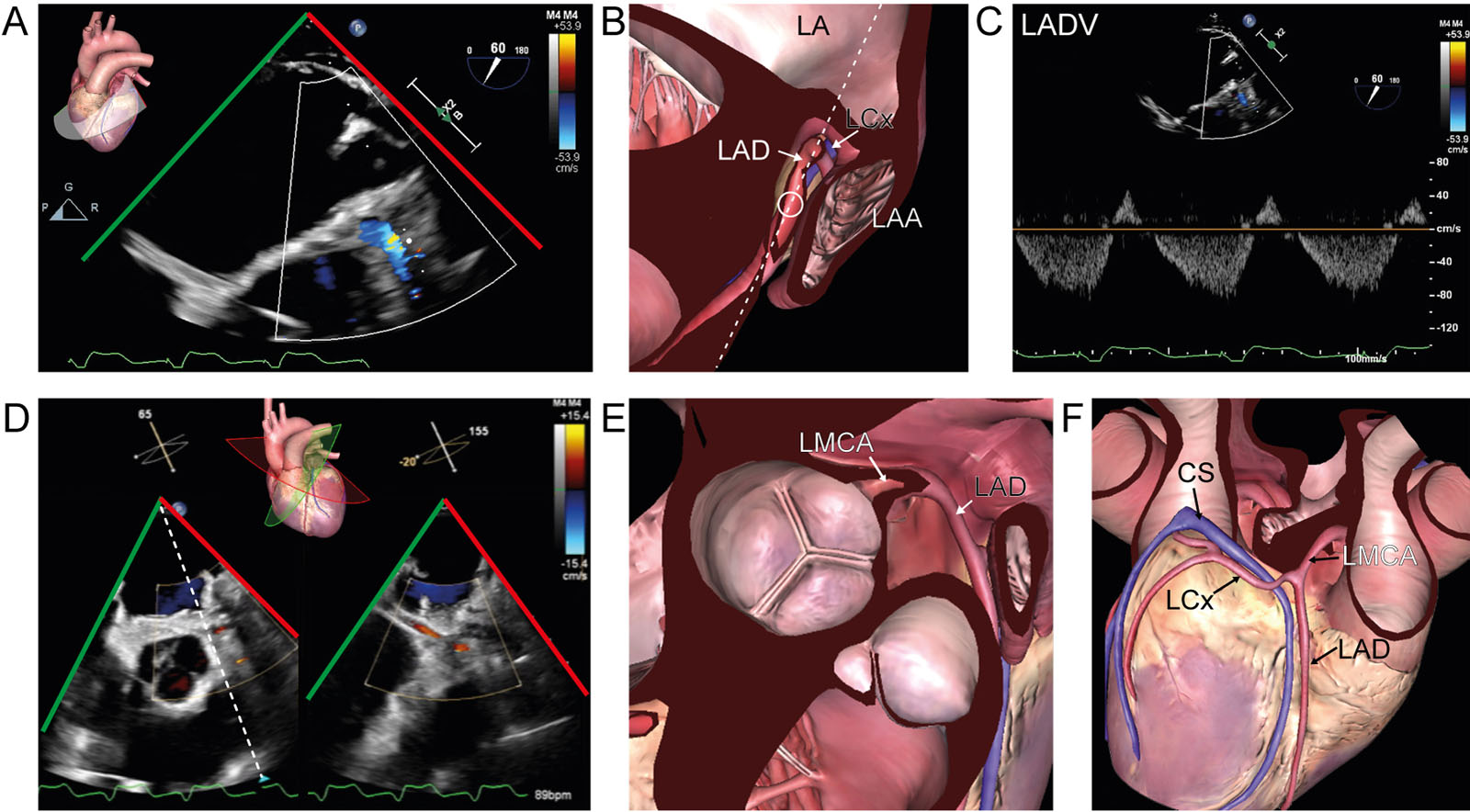
Coronary anatomy. (A, B) ME view at 60° with CFI in a 63-year-old woman after return on CPB for an inadequate LAD Doppler signal. (C) The PWD signal of the LAD has a predominantly normal diastolic velocities (normal: 71±19 cm/s). However, there is abnormal systolic reversal as cardiac function recovers from CPB. (D-F) ME AoV biplane view with CFI in a 59-year-old man after cardiac transplantation and graft failure. The LCx artery appears in both views with a normal CFI signal. Abbreviations: AoV, aortic valve; CFI, color flow imaging; CPB, cardiopulmonary bypass; CS, coronary sinus; LA, left atrium; LAA, left atrial appendage; LAD, left anterior descending; LADV, left anterior descending velocity; LCx, left circumflex; LMCA, left main coronary artery; ME, mid-esophageal; PWD, pulsed-wave Doppler.
Videos
Chapter 09 Fig01BC
Chapter 09 Fig02A
Chapter 09 Fig02C
Chapter 09 Fig03A
Chapter 09 Fig07AD
Chapter 09 Fig07B
Chapter 09 Fig07C
Chapter 09 Fig07D
Chapter 09 Fig11A
Chapter 09 Fig11B
Chapter 09 Fig11D
Chapter 09 Fig15
Chapter 09 Fig18
Chapter 09 Fig20D
Chapter 09 Fig20F
Chapter 09 Fig20I
Chapter 09 Fig21A
Chapter 09 Fig21C
Chapter 09 Fig22A
Chapter 09 Fig22C
Chapter 09 Fig22D
Chapter 09 Fig24A
Chapter 09 Fig24D
Chapter 09 Fig25A
Chapter 09 Fig25C
Chapter 09 Fig26A
Chapter 09 Fig26D
Chapter 09 Fig26E
Chapter 09 Fig27B
Chapter 09 Fig27D
Chapter 09 Fig28AB
Chapter 09 Fig28AC
Chapter 09 Fig28DE
Chapter 09 Fig28DF
Chapter 09 Fig29ABCDEF
Chapter 09 Fig30A
Chapter 09 Fig30D
Chapter 09 Fig31
Chapter 09 Fig32A
Chapter 09 Fig32Anew
Chapter 09 Fig33Bnew
Chapter 09 Fig33CDEnew
Chapter 09 Fig34B
Tables
eTable 9.5 Coronary angiography correlation with TEE
| C-Arm | Angiography | Simulation | TEE beam position | TEE view | TEE view | |
| Left coronary artery | ||||||
| A | RAO 10 Cranial 40  | 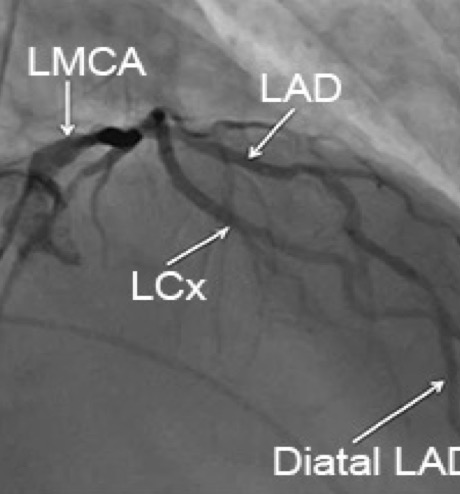 |  | 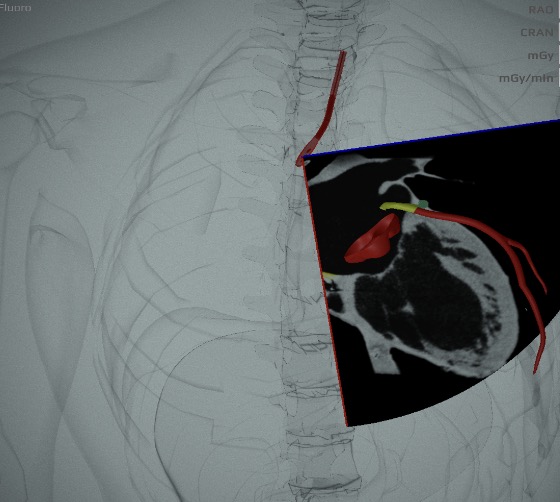 | ME 2C view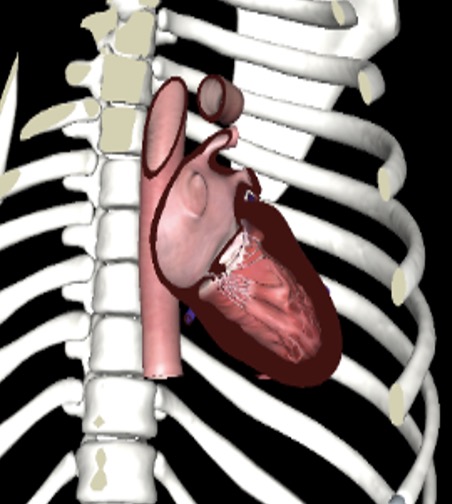 | 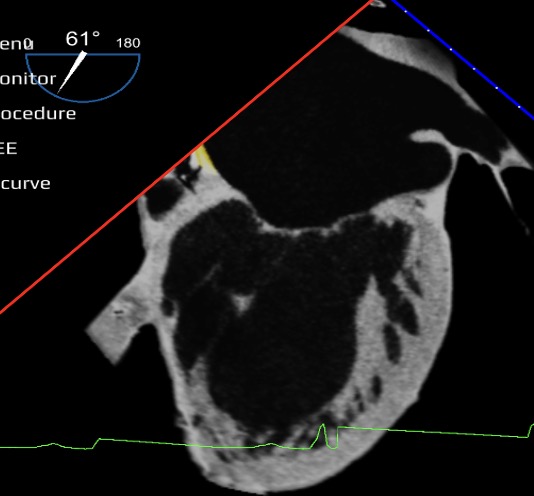 |
| B | RAO 15 Caudal 25  | 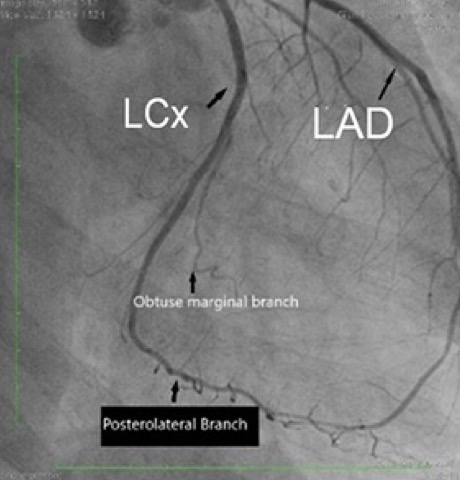 | 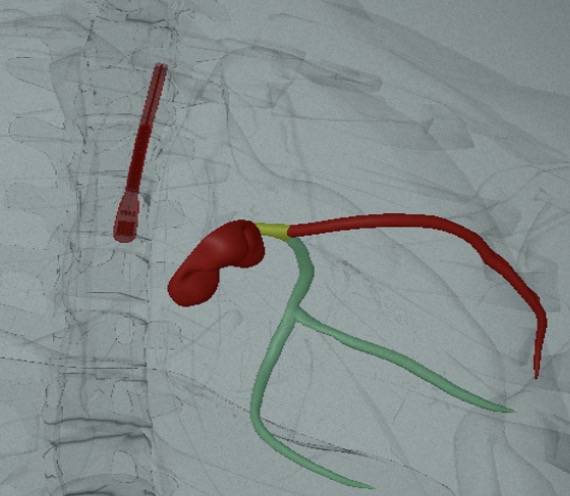 | 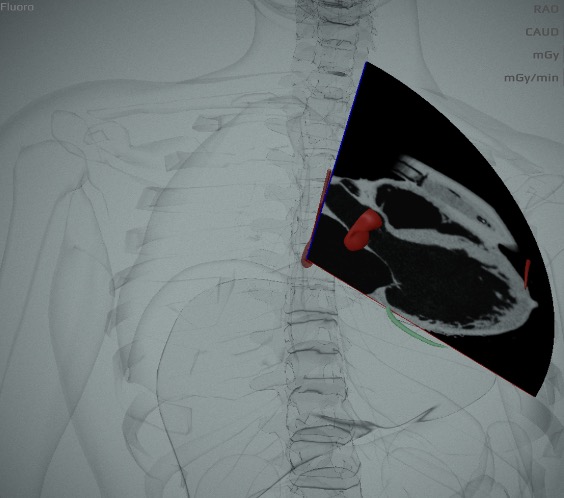 | ME 3C view 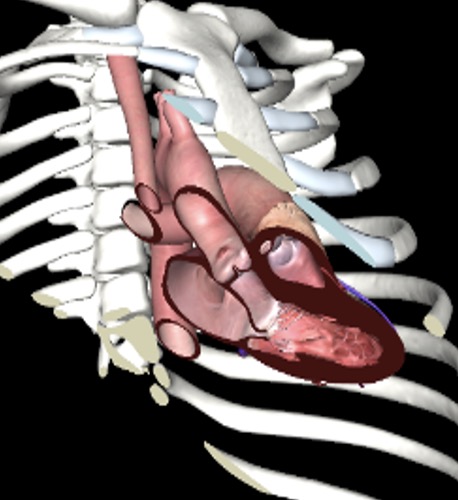 | 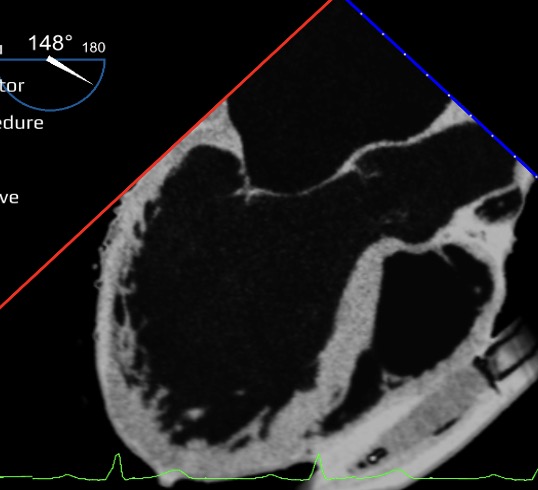 |
| C | LAO 45 Cranial 25 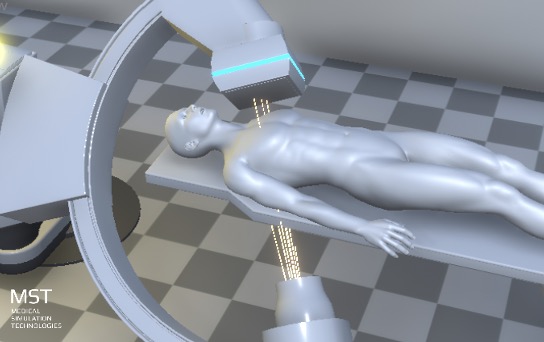 | 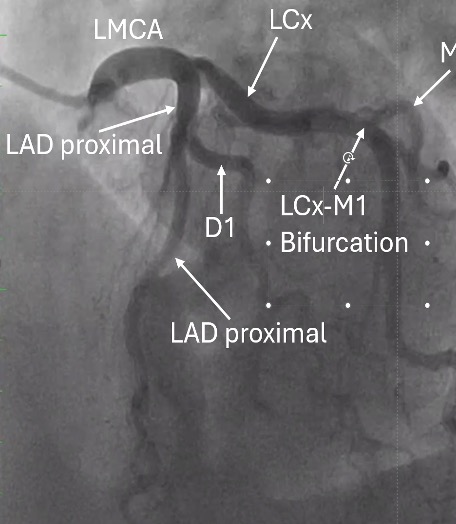 | 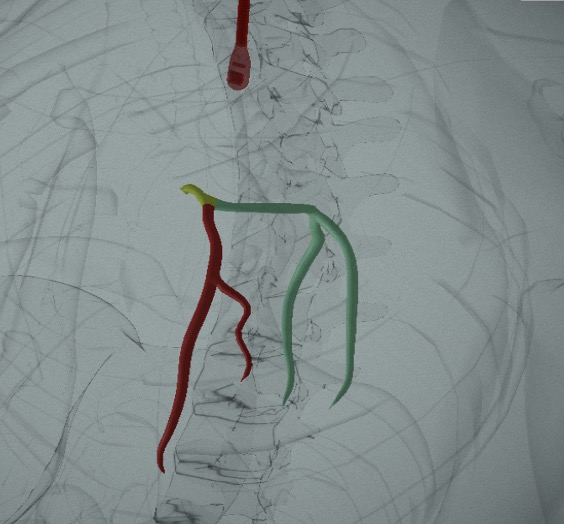 | 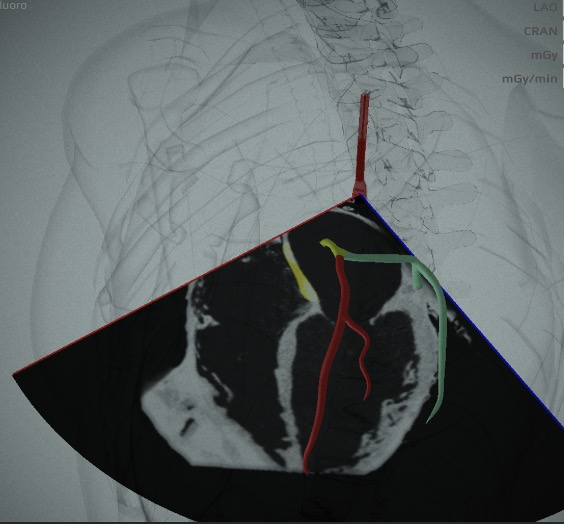 | ME 4C view  | 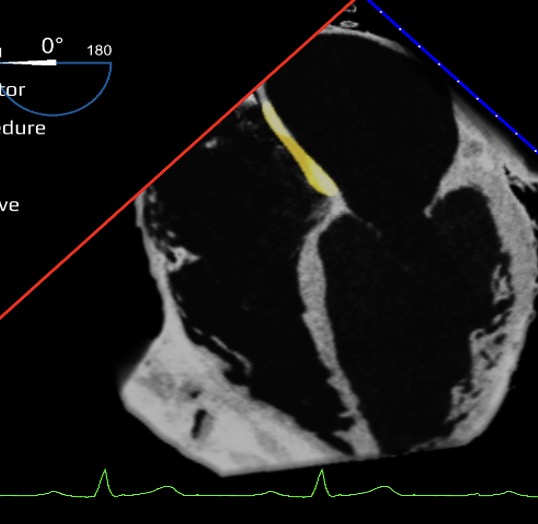 |
| D | LAO 25 Caudal 45 (Spider view)  | 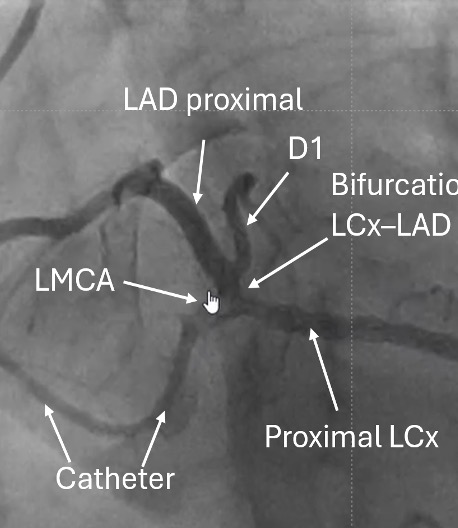 | 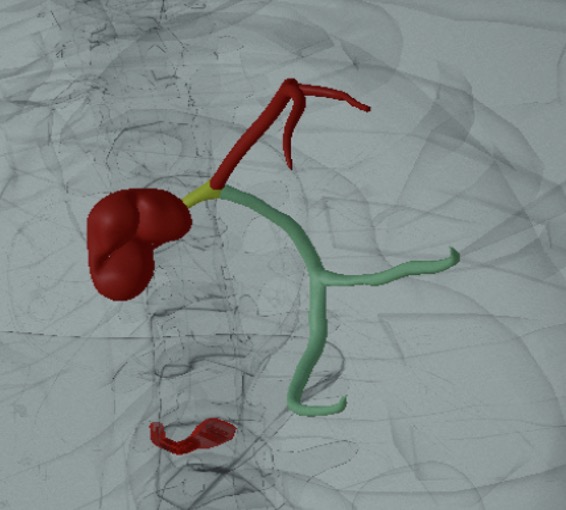 | 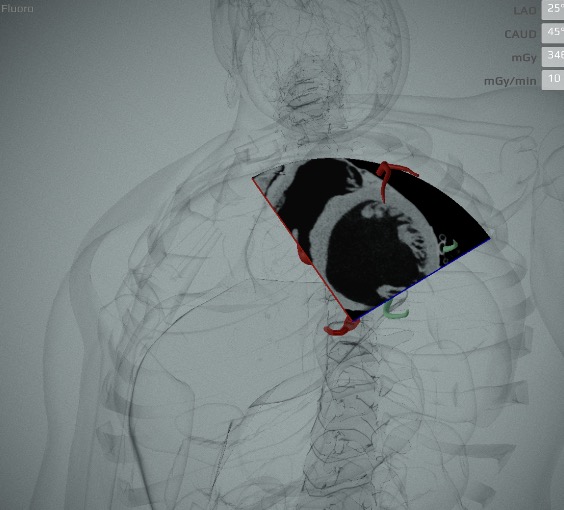 | TG SAX  |  |
| Right coronary artery | ||||||
| E | LAO 30 Cranial 0  | 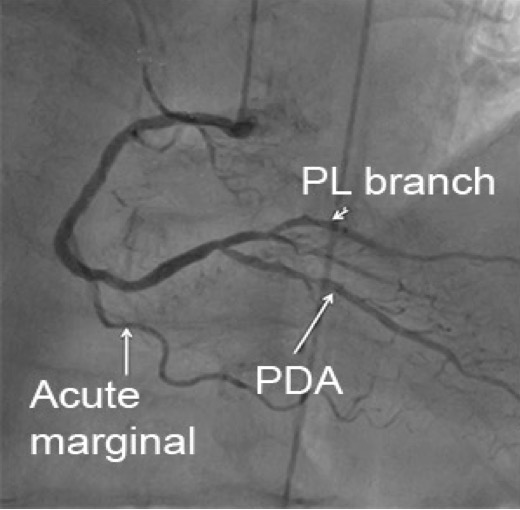 |  | 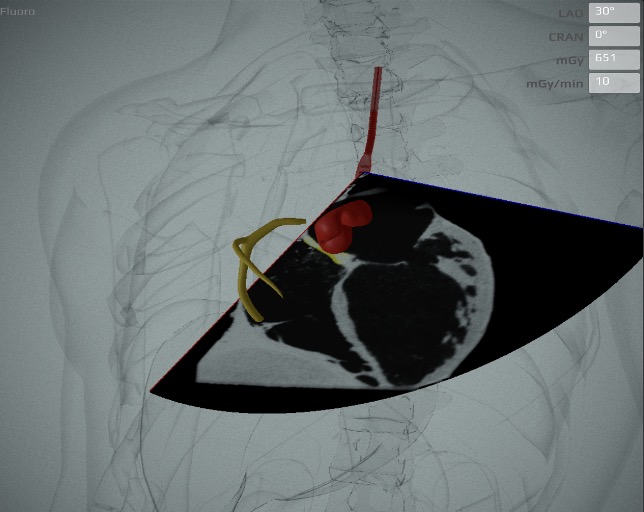 | ME 4C 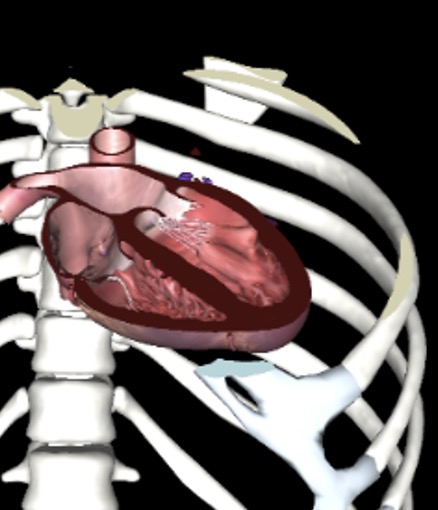 | 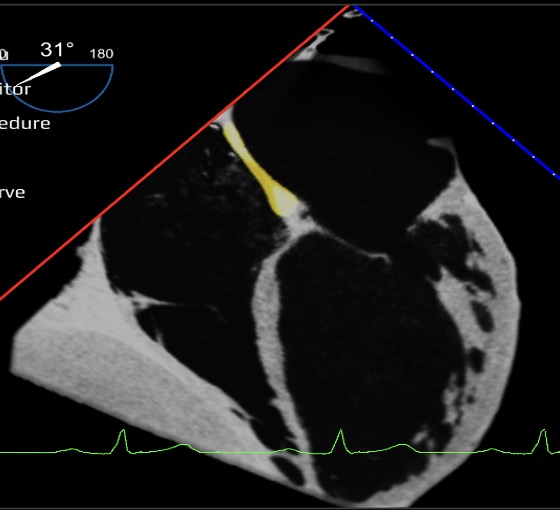 |
| F | RAO 30 Cranial 0 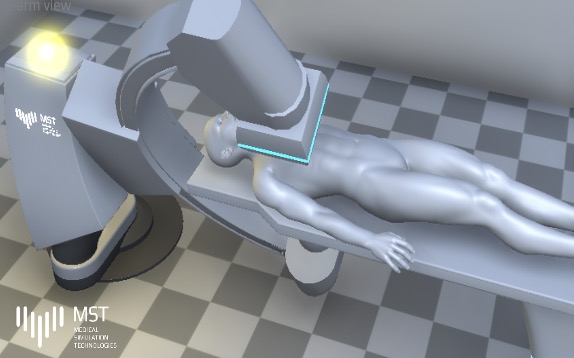 | 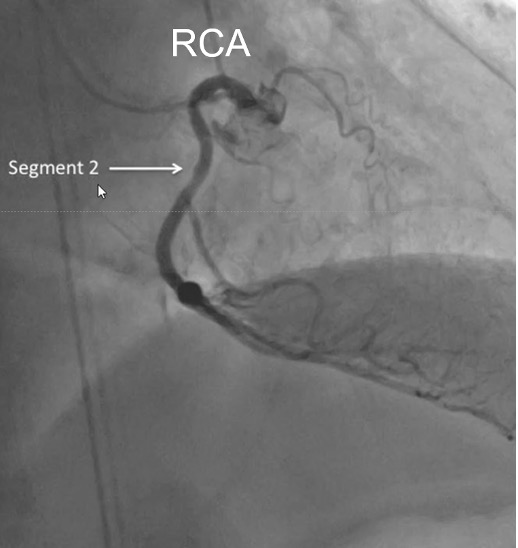 |  | 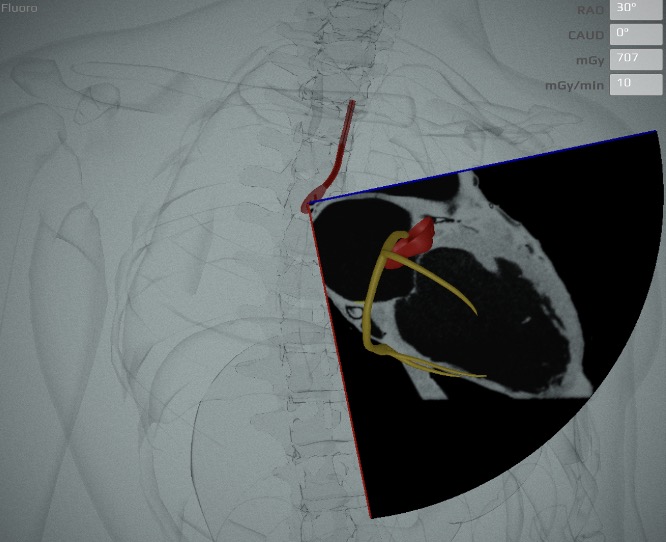 | ME 2C 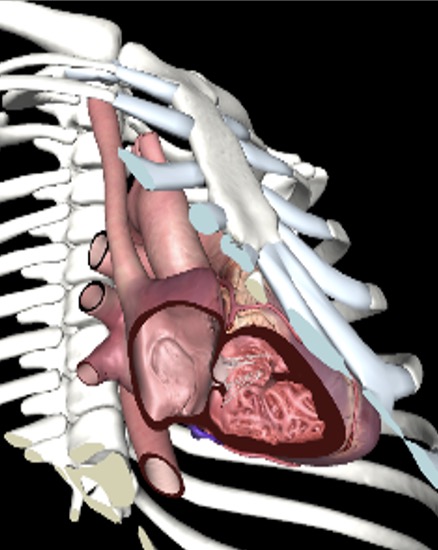 | 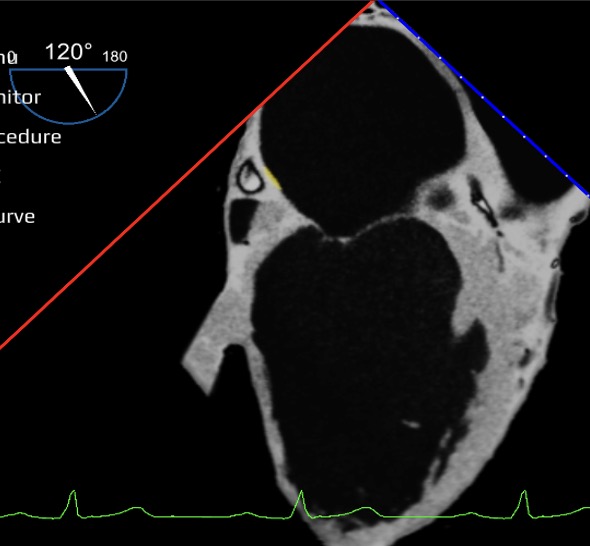 |
| Left mammary artery | ||||||
| G | LAO 90°  | 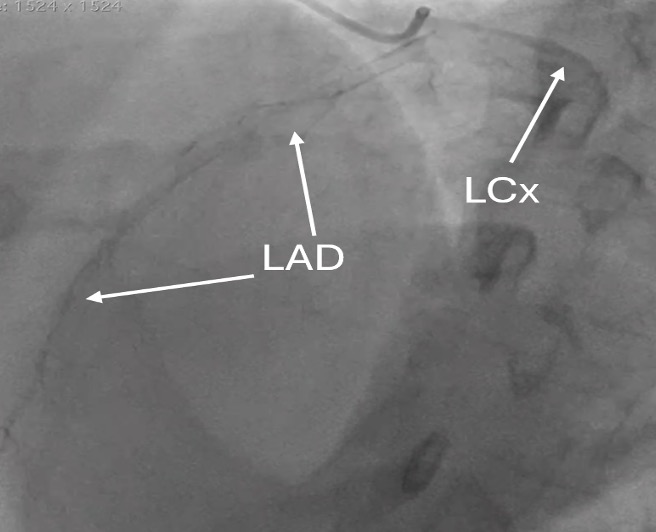 | 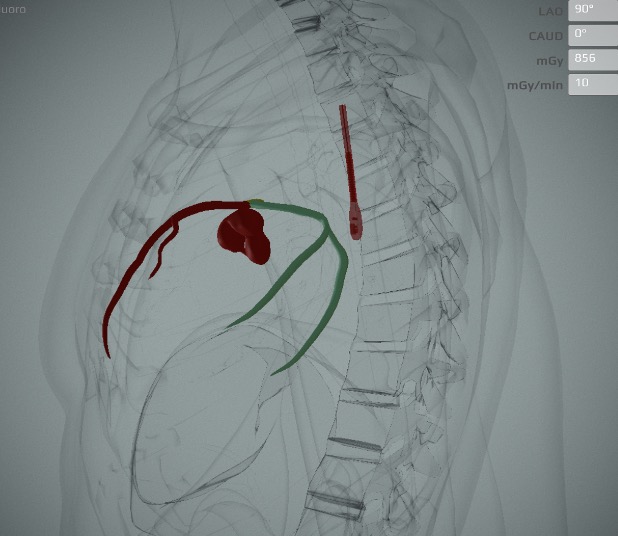 | 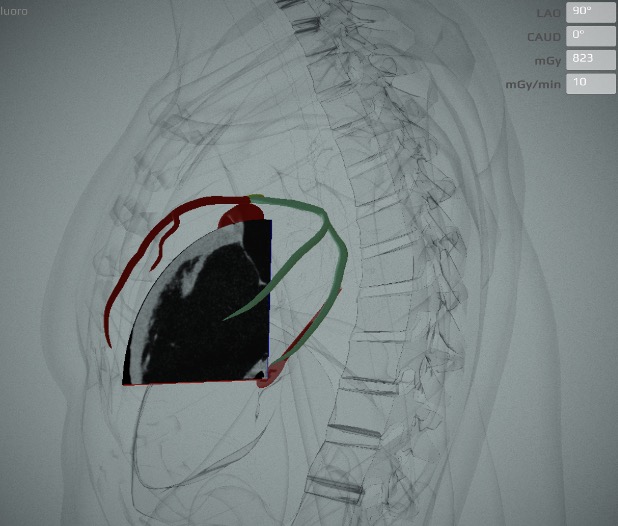 | 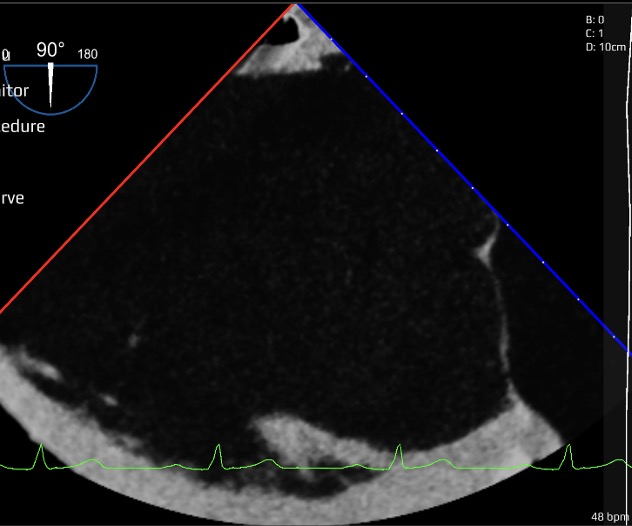 | |
A: RAO 10 Cranial 40. This is good view for LMCA and LAD-diagonal bifurcation. It corresponds to a ME 2C view; B: RAO 15 Caudal 25. This view is ideal for LCx branches visualisation. A codominant system is shown. It corresponds to a ME LAX view.; C: LAO 45 Cranial 25. This is good view for LAD and septal branches and ideal for diagonal artery visualisation. It corresponds to a ME 4C view; D: LAO 25 Caudal 45. The spider view is ideal for LMCA, LCx and LAD bifurcation and proximal LAD and LCx. It corresponds to a TG SAX; E: LAO 30 Cranial 0 is used to assess the 3 segments of the RCA, the PDA-PL bifurcation and the distal vascular bed. It corresponds to a ME 4C view; F: RAO 30 Cranial 0 will evaluate the upper knee and segment 2 of the RCA. It corresponds to a ME 2C view of the RV; G: LAO 90° view is used to see the mammary artery anastomosis.Abbreviations: | ||||||